Figure 1. Medial and Lateral columns of the posterior spine can be resected at varying timepoints.

Current Concept Review
1Department of Orthopedic Surgery, Vanderbilt University Medical Center, Nashville, TN; 2Department of Orthopaedic Surgery, Cedars-Sinai Medical Center, Los Angeles, CA; 3Department of Orthopedic Surgery, Akron Children’s Hospital, Akron, OH
Correspondence: Craig R. Louer Jr., MD, 2200 Children’s Way, Suite 4202, Nashville, TN 37212. E-mail: [email protected]
Received: December 19, 2022; Accepted: December 30, 2022; Published: February 1, 2023
Volume 5, Number 1, February 2023
Abstract
The posterior column osteotomy (PCO) is an adjunct technique for obtaining deformity correction during posterior spine fusion procedures. Full disarticulation of the posterior spinal column, including bony elements (namely the lamina and facet joints) and ligamentous complex is described as a PCO. This technique was originally described to allow for shortening of the posterior column during correction of excessive thoracic kyphosis; however, its indications have since been expanded to other spine deformities such as adolescent idiopathic scoliosis (AIS). Its expanded role in deformity surgery has been met with controversy: proponents tout increased flexibility and better spinal correction in three planes, while detractors cite lack of ostensible clinical benefit and potential for more complications. Differences in surgical technique are also prevalent. In this manuscript, we review the surgical technique of PCOs, including the traditional PCO as well as a modified posterior column release (PCR). Additionally, the controversy over when this technique should be utilized is further explored through summation of current literature on PCO outcomes.
Key Concepts
In 1945, Smith-Petersen originally described posterior column spinal osteotomies to correct kyphosis from ankylosed lumbar segments in rheumatoid arthritis. Complete facetectomy through both the superior and inferior articular facets corrected lumbar kyphotic deformity by transmitting leverage to the anterior column.1 In 1984, Alberto Ponte subsequently described a posterior column shortening osteotomy in the unfused thoracic spine to correct Scheuermann’s kyphosis. The “Ponte osteotomy” combines wide resection of the thoracic facet joints, laminae, and ligamentum flavum to generate 5-10 mm posterior gaps that close with compression through segmental instrumentation.2–5 Posterior column osteotomies (PCO) now are widely utilized for correction of hyper-kyphosis in the sagittal plane,5–9 as they allow an estimated 1 degree of kyphosis correction for every 1 mm of resection, resulting in up to 10 degrees of kyphosis correction per level.9,10
Indications for PCO have been expanded, including utilization with posterior spinal fusion (PSF) for correction of adolescent idiopathic scoliosis (AIS). The intended goal is to increase flexibility during three-dimensional deformity correction and restore normal sagittal plane parameters in the hypo-kyphotic thoracic spine by releasing the posterior tension band and lengthening the posterior column.11–15 However, the routine use of PCO for AIS remains controversial, with conflicting data as to the necessity, efficacy, and safety of this practice.16–18
Surgeon approach to PCOs is highly variable in AIS. While some surgeons utilize PCOs routinely in every AIS case, others use them sparingly. National trends are increasing, with utilization recently doubling from 17% of AIS cases in 2007 to 35% in 2015.19 Proponents say that PCOs improve correction in all three planes of deformity. In an era of increased attention on the sagittal plane and a focus on correction of thoracic hypokyphosis in AIS, some surgeons thus routinely perform PCOs to increase posterior distraction and thoracic kyphosis. Detractors argue that PCOs increase the risk of neurologic injury and do not impart a meaningful benefit for routine AIS cases.
There is also controversy regarding surgical technique. Ponte originally described wide posterior resection for posterior column shortening, commonly performed with a Kerrison, while some surgeons have transitioned to a modified approach with an ultrasonic bone scalpel (UBS). There are also differences in the chronology of performing PCOs during AIS surgery (whether prior to or after pedicle cannulation and screw placement). In this paper, we aim to highlight anatomic considerations and technical pearls for performing PCOs.
Thorough understanding of the posterior column anatomy of the thoracolumbar spine is critical to the performance of PCOs.
Ligamentous structures requiring disruption:
|
Bony structures requiring disruption:
|
The posterior spinal anatomy requiring resection for a PCO can be divided into medial and lateral structural elements (Figure 1). The posteromedial elements include the central lamina and the ligamentum flavum, while the posterolateral column is comprised of the superior and inferior articular facets. Temporally, the posteromedial and posterolateral columns may be addressed in varying order and at different points in the case to facilitate operative efficiency and safety. For instance, resection of the superior articular facets typically precedes pedicle screw insertion as screw heads may obstruct resection of the superior facet. However, the posteromedial column resection may be delayed until after pedicle screw insertion but immediately before rod insertion and deformity correction in order to reduce time that the spinal canal is exposed.
Figure 1. Medial and Lateral columns of the posterior spine can be resected at varying timepoints.
The traditional “Ponte-style” posterior column osteotomy for kyphosis dictates that symmetric gaps of 5-8 mm of the residual posterior elements are essential should be created in the posterior elements for uniform closure of the gaps with subsequent shortening of the posterior column. In severe or stiff deformities, Dr. Ponte advocated for wide resection from “pedicle to pedicle.”4
In hypo-kyphotic deformities (fixed lordosis or AIS), a similar posterior column “release” (PCR) has been described.20 This technique acknowledges that inducing kyphosis requires relative lengthening of the posterior column. The same anatomic structures must be addressed, though reducing the size of the resection gap may be preferred, thereby minimizing exposure of the underlying neural elements to theoretically decrease risk of neurologic injury and/or pseudarthrosis. This has been advocated by some to be done with use of an ultrasonic bone scalpel (UBS) for the benefit of minimal bone resection, decreased blood loss,20 and theoretical improvements in efficiency and safety. The authors’ preferred methods for both the traditional and modified release osteotomy will be described for the thoracic spine.
Figure 2. Sawbones representation of common level preparation for PCO. A) Every interspace in the operative field should have inferior facetectomies performed. B) Appearance following inferior facetectomy. C) Interspaces where PCOs will be performed will need spinous process and inferior lamina resection (colored in black), resulting in D) exposure of the superior articular facets (colored black) and ligamentum flavum (tan rectangle) for eventual resection and completion of PCO.
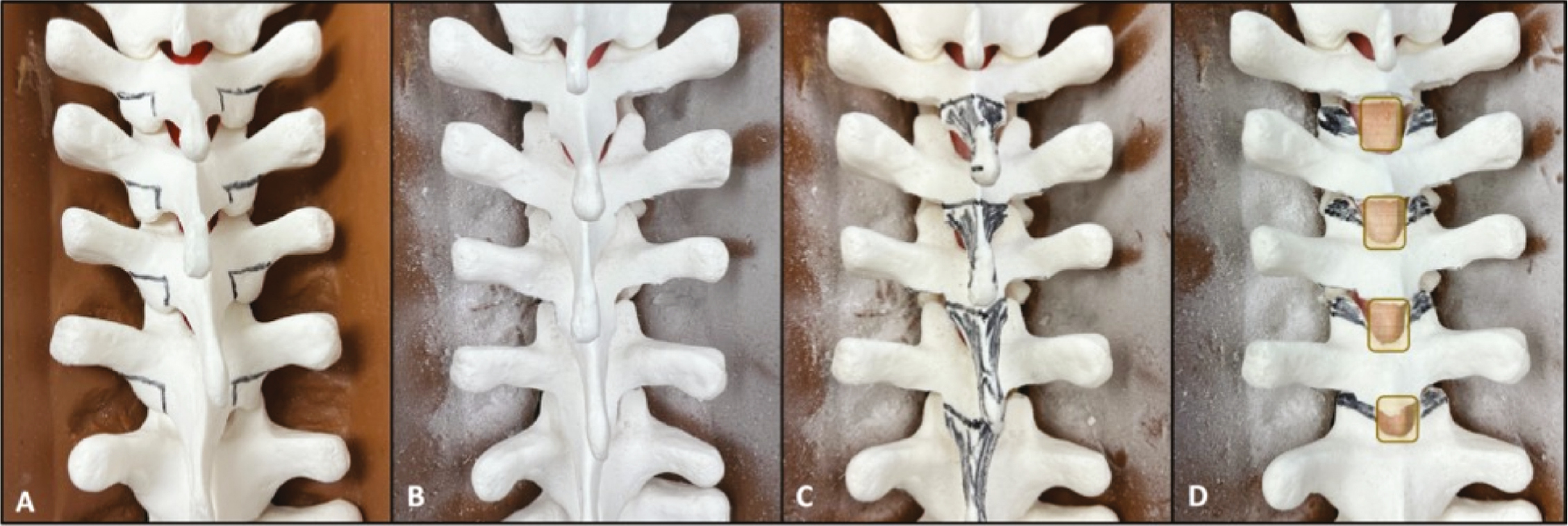
Figure 3. Surgical representation of common level preparation for PCO. A) Posterior spine following inferior facetectomies. B) Flexibility testing and deformity assessment to determine where PCOs may be beneficial. C) Removal of spinous process and inferior lamina at levels selected for PCO. D) Exposure of ligamentum flavum and superior articular facets following preparation steps.

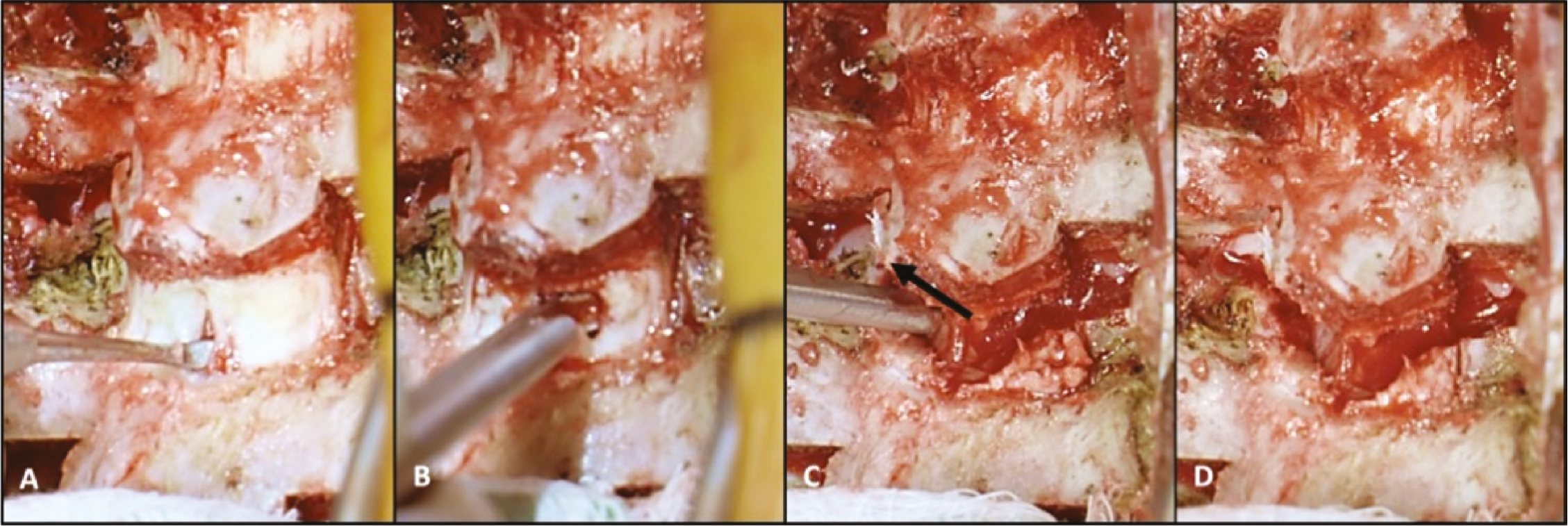
Figure 4. Method for Traditional Posterior Column Osteotomy (PCO). After thinning the ligamentum flavum (LF) with rongeur,
A) a Woodson elevator is used to palpate and dissect LF free from the epidural contents. B) Kerrison rongeur resects ligamentum flavum and C) superior articular facet bilaterally in a “V” shape. D) Completed PCO shows full disarticulation of the posterior spinal elements with symmetric gap for closure.
Following exposure, inferior facetectomies, and spinous process/lamina excision:
Figure 5. Method for Modified Posterior Column Release. A) Superior articular facets are cut with UBS prior to instrumentation. Following screw placement, the ligamentum flavum is resected starting with B) central resection with rongeur. C) Palpation/dissection with a Woodson elevator is performed prior to D) resection of ligamentum flavum with rongeur.
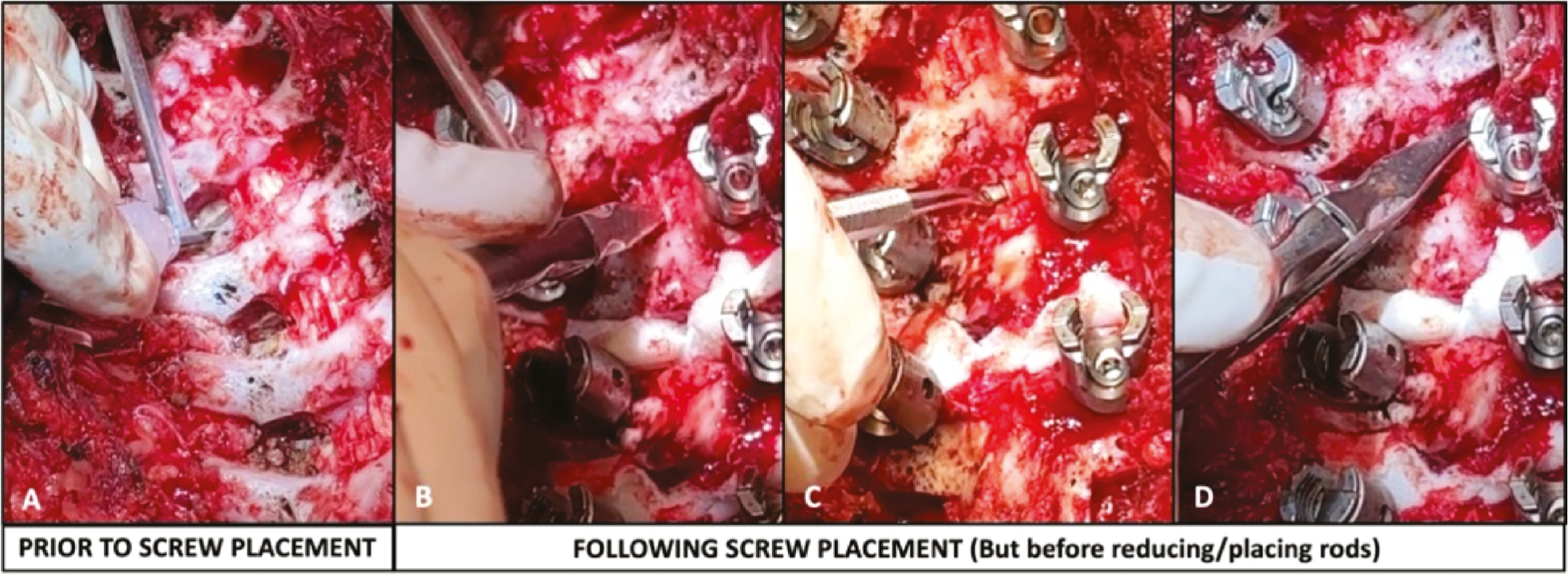
Figure 6. Placement of structural graft “strips.”

There have been highly variable reports of PCO outcomes. Many biomechanical studies demonstrate increased mobility from PCO with varying effects in each plane. Cadaveric studies comparing PCOs to specimens with intact facets found that PCOs reduce axial-plane derotational forces by 18%,22 while sequential PCOs improve flexion (+1.6°/osteotomy), extension (+1.5°/osteotomy), and axial rotation (+2.8°/osteotomy) with little effect on lateral bending motion.23 Likewise, Wang et al. concluded that PCOs increase flexibility in the axial and sagittal planes but have little effect on coronal correction, and overall gains are less effective than anterior releases.24 Interestingly, Holewijn et al. found 29.6% improvement in flexion and axial rotation after resection of the interspinous ligament, inferior facets, and ligamentum flavum, but sequential superior facetectomy provided no biomechanical benefit, thereby demonstrating the “law of diminishing returns.”17
Clinical results are even more variable, likely associated with difficulty isolating independent variables as many covariates may affect correction, including clinical factors such as gender, age, curve magnitude, and stiffness, and technical factors like rod material, rod size, implant type, implant density, deformity correction technique, and surgeon. The first large single-center cases series reporting the results of PCO to restore kyphosis in the hypokyphotic thoracic spine demonstrated increased T5-T12 kyphosis from 8 degrees to 18 degrees, and these AIS patients had 6% increased coronal correction with 8% IONM critical changes, but lacked a comparison group.14 Samdani et al. subsequently compared 125 Lenke 1 AIS patients with 4.3 ± 1.5 PCO to 66 unmatched controls and found that PCO improved the correction index from 62% to 67%, for a 3.3 degrees coronal plane improvement, 3.5 degrees kyphosis improvement, 15% rib prominence correction, though similar SRS scores.15
Other clinical studies have demonstrated little benefit from PCOs but potentially increased surgical risk. An unmatched comparison of AIS patients with and without PCO found no significant difference in coronal plane correction or kyphosis restoration while estimated blood loss (EBL) was 33 ml/level higher and operative time 8 min/level longer in the PCO group.16 In a single-center matched cohort of 68 patients, PCO provided no improvement in the sagittal or axial planes, only 8% improvement in coronal plane correction, and higher risk of critical neuromonitoring changes (15% with PCO vs. 0% without, p=0.05) with no difference in health-related quality of life (HRQoL).18
Other studies have likewise identified PCOs as an independent risk factor for intraoperative neuromonitoring (IONM) changes.25,26 Buckland et al. found that PCOs are an independent risk factor for IONM alerts (9.3% vs. 4.2%, p<0.001), though this did not manifest into a significantly different incidence of postoperative neurologic deficit (0.37% with PCO vs. 0.17% without, p=0.45).25 A large, unmatched, multicenter database study reported that patients with PCOs have higher risk of readmission and reoperation within 90 days but similar reoperation rate within 2 years while PCOs incur increased procedural cost resulting in a $15,854 higher mean hospital cost.19
Posterior Column Osteotomies (PCOs) for spine deformity surgery have controversial indications with debated outcomes. There are varying technical approaches for PCO performance, with traditional PCO and modified posterior column release (PCR) both having been described in the literature. Prospective randomized studies are needed on clinical outcomes for standard PCOs and the varying technical modifications.
C. Louer: Consultant – Depuy Synthes Spine; Research Support – NuVasive Spine – Shared support for research personnel, POSNA Zimmer Biomet Spine Research Grant; Royalties – Nsite Medical, Inc.; K. Illingworth: Consultant – Orthopediatrics; T. Metcalf: Position supported by NuVasive Spine educational grant; L. Flocarri: Nothing to disclose.