
Master’s Surgical Technique
Removal of Femoral Lengthening Nails
1Department of Orthopedic Surgery, Nationwide Children’s Hospital, The Ohio State University, College of Medicine, Columbus, OH; 2Department of Orthopaedics, Aalborg University Hospital, Aalborg, Denmark
Correspondence: Christopher Iobst, MD, FAOA, Nationwide Children’s Hospital, Department of Orthopaedics, 700 Children’s Dr., Columbus, OH 43205. E-mail: [email protected]
Received: March 15, 2022; Accepted: March 25, 2022; Published: May 1, 2022
DOI: DOI: 10.55275/JPOSNA-2022-0031
Volume 4, Number 2, May 2022
Abstract:
“No surgeon ever looks good taking out hardware.” This simple statement illustrates the frustration many of us have felt when faced with an implant removal case. Since all internal lengthening nails are recommended for removal at the completion of treatment, any surgeon considering a patient for internal lengthening will eventually encounter a nail removal opportunity. As part of our limb reconstruction practices, the authors have removed hundreds of internal lengthening nails. We have developed techniques through trial and error over time to streamline and simplify the nail removal process. The goal of this article is to share our experience with you in the hopes that it makes your internal lengthening femoral nail removal surgery as smooth and painless as possible.
Key Concepts:
- Do not remove all the interlocking fixation elements before securing the nail to the retrieval device.
- Rotate the limb until the fixation elements are in profile under fluoroscopy. This will best determine if there is bone overgrowth that will prevent percutaneous removal of the interlocking elements.
- Remove any bone or debris over the tip of the nail with a reamer. The reamer size should be at least 1 mm larger in diameter than the largest diameter of the nail to be retrieved.
- For retrograde nail removal, a bump should be placed until the knee to create a straight, continuous line to the nail, where the patella is out of the path.
Introduction
There are currently two main femoral lengthening nails on the market, the Precice magnetic lengthening nail (NuVasive, San Diego, CA) and the motorized Fitbone® lengthening nail (Wittenstein intens, Igersheim, Germany). Although the removal techniques are similar for each nail, we will try to highlight the specific nuances that are unique to each nail type.
Antegrade Intramedullary Lengthening Nail Removal
Patient positioning is an underrated but critical step in nail removal surgery. Having the patient in the proper position initially helps to make the rest of the surgery go smoothly. Conversely, an improperly positioned patient can create a frustrating and difficult surgical experience. Depending on the surgeon’s preference, antegrade nails can be removed in either the supine or lateral decubitus position.
Positioning: Supine
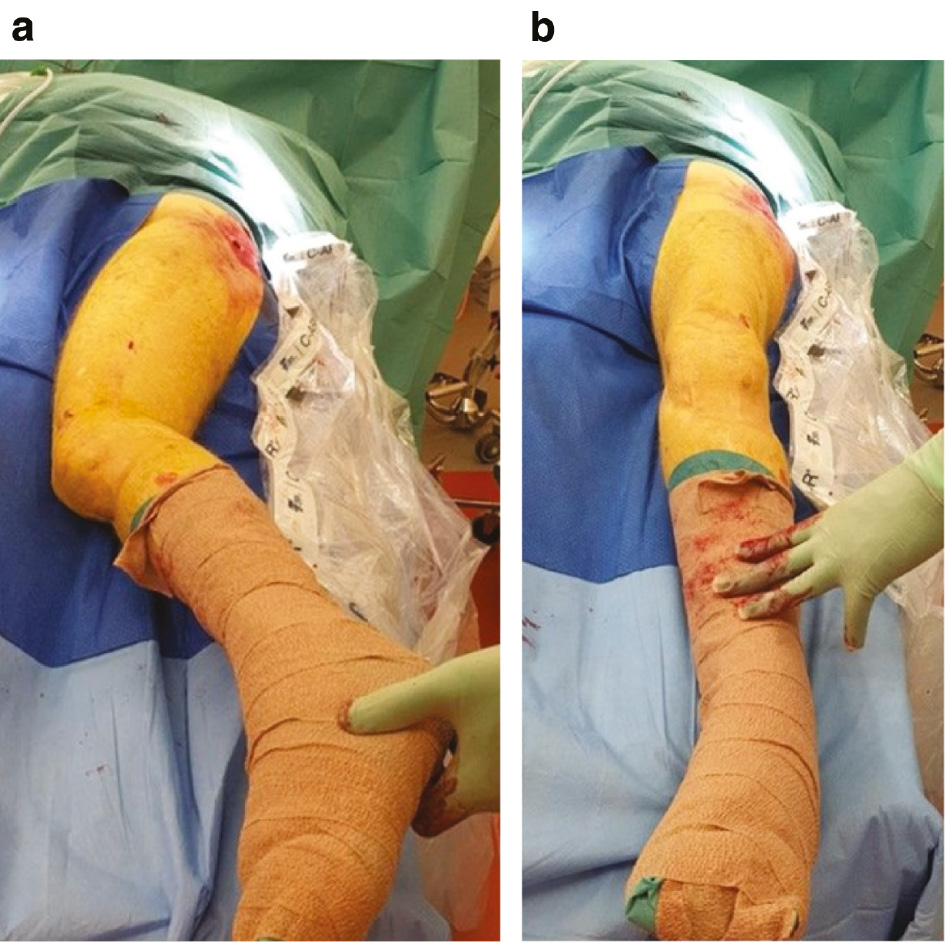
The patient should be placed on a radiolucent table as close to the edge of the table as possible. The ipsilateral arm must be secured across the chest (Figure 1). This arm position is critically important to allow the surgeon the necessary space to work. In order to be in the proper position to remove the nail from the proximal femur, the surgeon will need to approach the gluteal region from the direction of the patient’s torso. The lower extremity can also be slightly adducted to improve access to the gluteal region. A small bump is placed under the ipsilateral hemi-pelvis to slightly lift the hip off the table. The bump improves the quality of the fluoroscopic image in the lateral view. After the entire limb is prepped, split drapes are used to keep the gluteal region up to the iliac crest exposed and visible (Figure 2). There should already be a gluteal incision from the nail insertion that can be used as a guide for the extent of draping exposure required. Ioban drape can be used to seal the edges of the drapes and prevent loosening of the drapes during surgery.
Figure 1. Proper positioning of the patient is critically important. The patient should be placed on a radiolucent table as close to the edge of the table as possible. The ipsilateral arm must be secured across the chest.

Figure 2. After the entire limb is prepped, split drapes are used to keep the gluteal region up to the iliac crest exposed and visible.

Positioning: Modified Lateral
Alternatively, the patient can be placed in a modified lateral position on a radiolucent table. This allows AP and lateral views to be taken without having to rotate the fluoroscopy machine around the patient. For this position, the patient is secured on the table with a wedge (triangle) pad placed posteriorly at the level of lumbar column and pelvis. This positions the limb at about 45 degrees to the plane of the bed. Rotating the limb 45 degrees internally will allow a lateral view and rotating 45 degrees externally will produce an anteroposterior view (Figure 3a and 3b). The surgeon will need to approach the gluteal region from the direction of the patient’s torso to be in the proper position to remove the nail from the proximal femur. The lower limb that is not operated on can be secured to the table by a strap around the leg and the table. The limb to be operated on should be mobile on the table. The operated extremity can be slightly adducted by positioning it in front of the other leg to improve access to the gluteal region. The limb is prepped from distal to the knee joint and split drapes are used to keep the gluteal region exposed and visible. There should already be a gluteal incision from the nail insertion that can be used as a guide for the extent of the proximal draping exposure required.
Figure 3a (left) and 3b (right). The modified lateral position allows the limb to be rotated from a lateral (3a) to an anteroposterior position (3b) without having to change the orientation of the fluoroscopy machine.
Nail removal (Precice Magnetic Nail)
- Distal interlocking screw/peg removal
After the patient is properly positioned, prepped, and draped, fluoroscopy is used to identify the location of the distal interlocking screws/pegs. Rotate the limb until the fluoroscopy beam hits the pegs/screws in profile orthogonally (Figure 4). Key Tip: By rotating the limb in this way you are able to determine if the pegs/screws are covered with bone and also insertion of the screwdriver orthogonal to the x-ray beam and in-line with the screw trajectory helps direct the screwdriver into the screwhead. Since most nails are designed to be removed within 9-12 months of insertion, there usually isn’t substantial bone overgrowth over the peg/screw heads. Leaving the screw/peg head slightly proud on purpose at the time of insertion will make it easier to palpate and capture at the time of removal.
If there is evidence of bone overgrowing the peg/screw heads, then a more extensive approach to the lateral femur will be necessary to access the pegs/screws under direct vision. A combination of curved osteotomes and curets can be used to carefully remove the overlying bone. Avoid overly aggressive curettage of the opening in the peg/screw head as the interior threads may become damaged. This will prevent the threaded retrieval device from being able to fully capture the peg/screw head.
If the distal interlocking screws/pegs still line up with their insertion incision, then the same incision site is opened. If the screws have migrated distally due to the lengthening, then a separate, 1 to 2 cm incision should be created centered over the space between the two screws/pegs. A straight hemostat can be used to percutaneously dissect down to the screw/peg heads. Key Tip: The straight hemostat is easier to use than a curved hemostat because it creates a straight path from the skin to the peg/screw that can be followed by the straight screwdriver handle. The straight hemostat can be inserted into the head of the peg/screw to clear any soft tissue and to provide the surgeon with a visuo-spatial guide to finding the peg/screw head percutaneously with the screwdriver.
The cannulated screwdriver with the threaded cannula can then be inserted into the peg/screw head following the same path. The screwdriver must be in the exact orientation of the peg/screw head for the threaded cannula to properly capture the threads inside the peg/screw head (Figure 5). Fluoroscopy can assist with finding the perfect alignment of the screwdriver with the peg/screw head. Once the threaded portion of the screwdriver is engaged in the screw/peg, a half turn tightening the peg/screw (clockwise turn) will help to loosen it and prevent stripping of the peg/screw. Since the pegs only have proximal threads, the maneuver for their removal is a combination of turning counterclockwise (to back up the threaded portion of the peg) while simultaneously pulling the peg out of the patient (to retrieve the smooth portion of the peg).
- Capture the proximal nail end
Once each of the two distal interlocking screws/pegs (or in special cases, three distal interlocking screws) has been removed, the next step is to capture the proximal end of the nail. Key Tip: The nail needs to be captured prior to removing the proximal interlocking screws/pegs so the retrieval guide can be screwed into the nail while it is still secured to the bone without inadvertently driving the nail further into the bone.
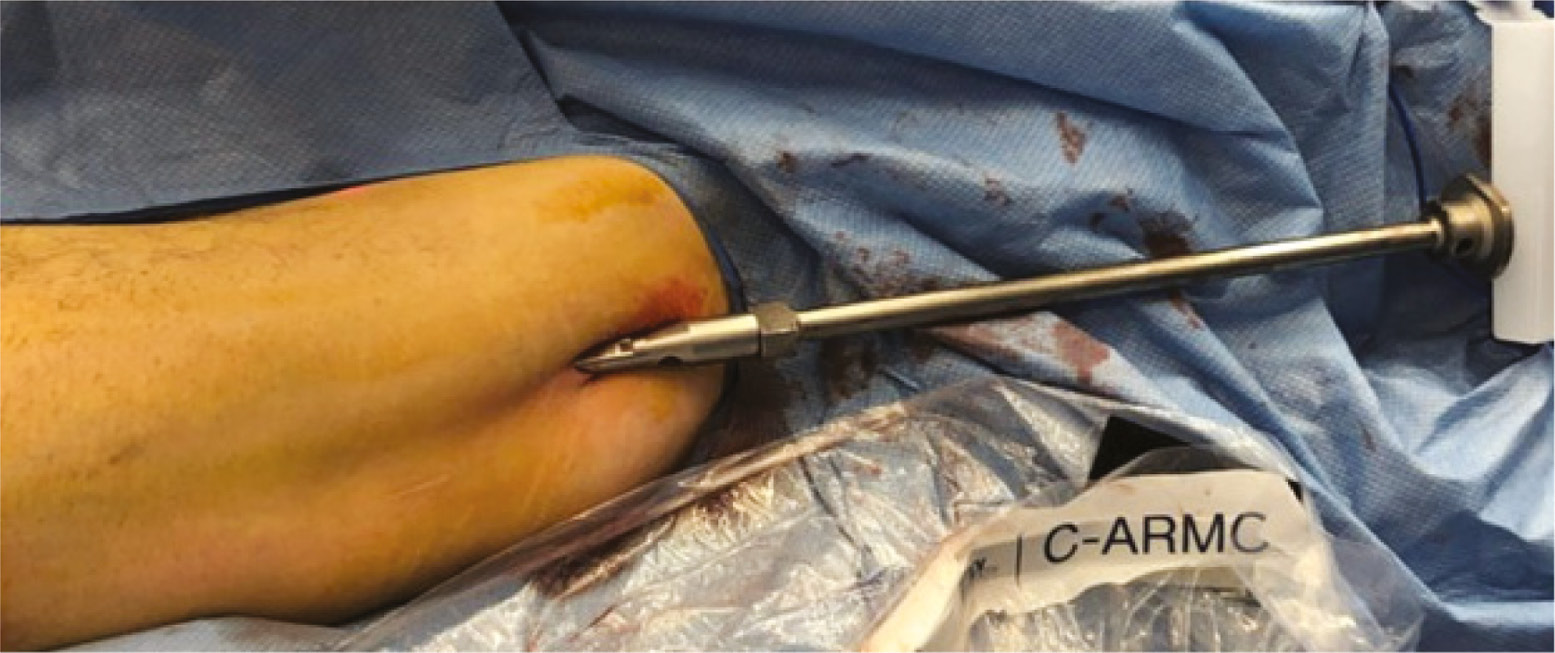
The gluteal incision for insertion of the nail can be opened approximately 2 cm and a 3.2 mm guidewire is carefully inserted towards the greater trochanter or the piriformis fossa under fluoroscopic guidance (Figure 6). The goal is to aim the wire towards the center of the proximal end of the nail in both the coronal and sagittal planes (Figure 7a and 7b). Once it is aligned, it can be tapped with a mallet into the nail until it is fully seated (Figure 8). If orthogonal views from fluoroscopy confirm the wire is in the proper position, a cannulated reamer is passed over the wire down to the proximal tip of the nail (Figure 9). A Kelly hemostat can be used to spread the tissue wide enough to allow the reamer to slide easily to the nail. Key Tip: The reamer size should be at least 1 mm larger in diameter than the largest diameter of the nail to be retrieved. The reamer is activated and any bone covering the tip of the nail is cleared away (Figure 10). This usually requires activating the reamer for only a few seconds. Carefully remove the reamer without pulling the guidewire out of the tip of the nail. Detaching the reamer from the power source and using an obturator may be necessary to ensure the wire stays in place. If the wire is inadvertently pulled out of the nail, it can be re-inserted percutaneously with fluoroscopic guidance. However, spending a few extra seconds to ensure the wire stays in place will save operative time and eliminate extra fluoroscopic exposure to the patient and the surgeon. A cannulated retrieval device can then be passed over the guidewire directly into the proximal end of the nail (Figure 11). Verify that the retrieval device is parallel to the end of the nail in both the coronal and sagittal planes prior to tightening it. The retrieval device should turn smoothly and capture at least 5 mm of thread within the nail (Figure 12). A tommy bar can be inserted into the retrieval device to allow more torque with turning of the retrieval device to ensure it is fully engaged and tight. Key Tip: Use of a reamer is critical to clear soft tissue and bone away from the proximal end of the nail to ease threading of the retrieval bolt.
- Proximal interlocking peg/screw removal
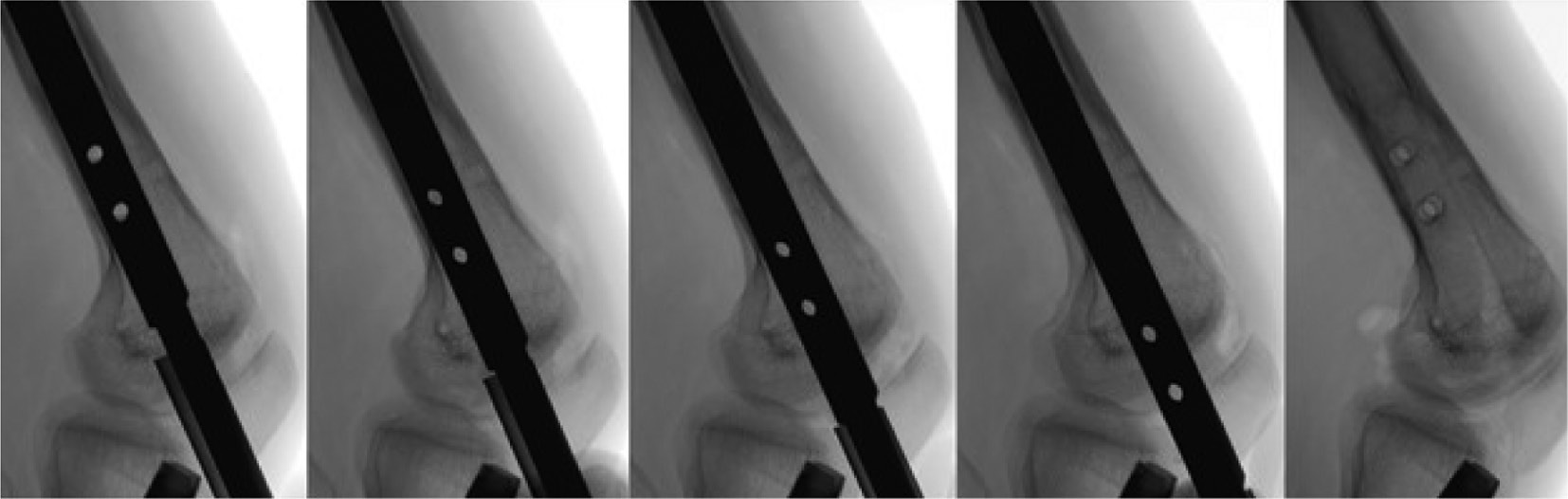
When the nail has been captured with the retrieval device, the proximal interlocking screws/pegs can be removed. These screws/pegs are typically still in the same position as they were at the time of insertion. Therefore, the original incision used for insertion can be used for removal. Like the distal interlocking screws/pegs, the limb can be rotated under fluoroscopy until the peg/screw heads are seen in profile to determine if there is any bone that has grown over the tips of the screws/pegs. A straight hemostat can be used to palpate the peg/screw heads and clear any soft tissue from inside the peg/screw head. The cannulated retrieval device is then attached percutaneously to each screw/peg and they are removed in the same manner as the distal interlocking screws/pegs.
- Nail removal
If all the distal and proximal interlocking elements have been removed, the nail can be removed from the canal. A cannulated impactor can be attached to the retrieval device (Figure 13). Spending a few seconds, scanning the entire length of the nail with the fluoroscope can ensure that all interlocking screws have been removed and prevent a devastating fracture occurring from locking screws still in place. Key Tip: Rotate the well-fixed retrieval device clockwise and ensure during fluoroscopy that the locking holes, and thus the nail, rotates freely prior to extraction. It is important to rotate the retrieval device clockwise to prevent detachment between the nail and the retrieval device. In some cases, the nail can be rotated and pulled out by hand. However, the nail can also be gently removed using a slotted mallet over the impactor. Adducting the limb will help to clear the path for the nail to be removed from the tissues. Carefully retract the soft tissues to allow the proximal tip of the nail to clear the skin smoothly. Over-aggressive mallet swings during nail removal can cause a fracture to the proximal femur or femoral neck. Once the nail is fully removed, fluoroscopic images should be obtained to verify the entire femur shaft and neck, including the regenerate bone, is intact.
Figure 4. Rotate the limb until the distal interlocking elements are in perfect profile. This will help determine if there has been any bone growth over the top of the fixation elements that might preclude a percutaneous removal attempt. It is additionally advised to use this position to remove the screw. Placing the screwdriver in-line with the screw in perfect profile and perpendicular to the fluoroscopy beam will ensure proper orientation and facilitate engagement into the screw head.

Figure 5. Capturing the fixation element with the threaded removal device allows percutaneous removal.
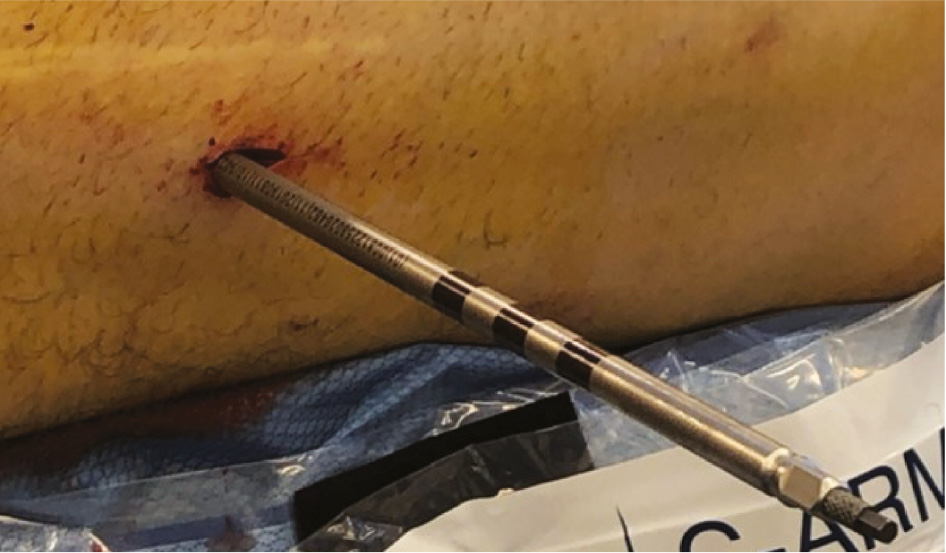
Figure 6. Percutaneous placement of a guidewire for antegrade nail removal.

Figure 7a (left) and 7b (right). Carefully advance the guidewire under fluoroscopic guidance into the center of the nail on the anteroposterior view (7a) and the lateral view (7b).
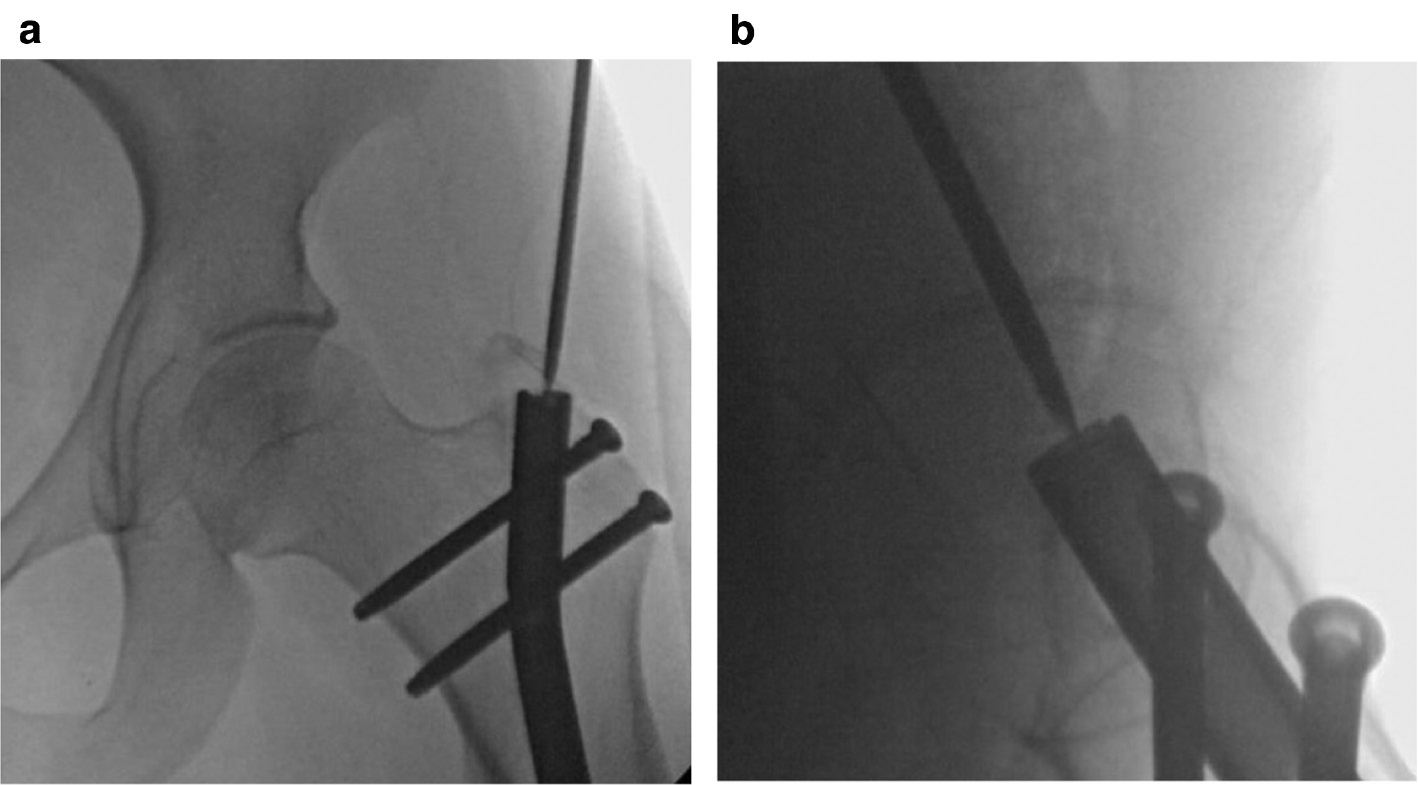
Figure 8. Tap the guidewire with a mallet into the proximal end of the nail. If one looks carefully, they can see heterotopic bone over the proximal end of the nail. Reaming the muscle and bone over the nail will develop a clear path for threading in the extraction bolt.

Figure 9. Make a 2 cm incision to introduce a reamer over the guidewire and remove any bone over the top of the nail. The reamer should be at least 1 mm larger than the diameter of the nail.

Figure 10. Fluoroscopic image demonstrating the reamer down to the proximal tip of the nail.
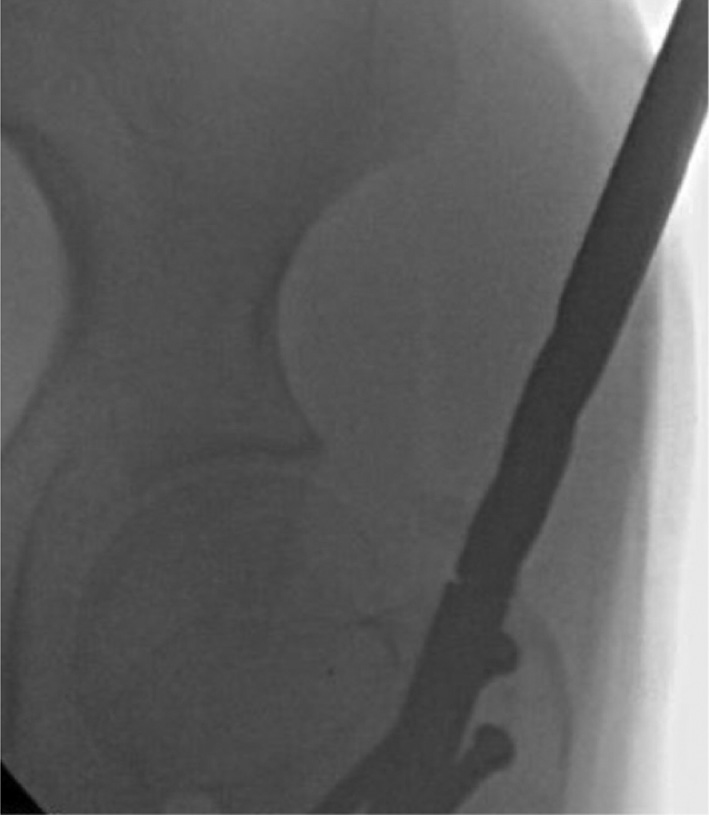
Figure 11. Maintain the guidewire in the tip of the nail after reaming. This allows a cannulated removal bolt to be inserted directly into the proximal tip of the nail.

Figure 12. Fluoroscopic image demonstrated the threaded retrieval device capturing the proximal portion of the nail.

Figure 13. A cannulated impactor is attached to the threaded retrieval device.
Nail Removal (Fitbone® Motorized Nail)
- Similar to the magnetic nail, the single distal interlocking screw is removed first from the Fitbone® motorized nail (Figure 14). Note that the motorized nail only has one interlocking screw to remove as opposed to the magnetic nail which can have up to three interlocks.
- The next step is unique to motorized nails and involves removing the receiver. The original incision can be used to locate the cable. Dissect subcutaneously towards the connector and the receiver. Once the cable is identified, it is cut between the connector and the nail (Figure 15). The receiver with the connector can be removed as a unit. The remaining cable extending from the inside of the nail can now be removed by pulling on it by hand or with a hemostat, as it usually breaks off inside the nail.
- A 3.2 mm K-wire is used to guide the direction of the nail removal path. It should be placed through the fascia and centrally into the proximal end of the nail in both planes. The leg usually needs to be adducted to achieve the correct direction of the K-wire.
- The fascia is divided with a scalpel along the K-wire and the 12 mm cannulated cone is inserted. If the nail is buried in the bone, the cannulated reamer can be used to remove overlying bone. The entire narrow portion of the cone must be tapped into the bone by the hitting device for cone insertion. The medium size 13/12 mm tube can now be placed over the cone. It can be recessed into the bone by using the hitting device for tube insertion. Be careful to avoid touching the nail with the tube to prevent damaging the tube.
- When the cone is tightly inserted in the bone, the cannulated nail retrieval device can be attached to the nail by turning it clockwise and tapping at the same time until the thread is fully inside the nail and cannot turn anymore.
- The proximal locking screws are now removed (as described for the magnetic nail).
- The entire length of the nail is scanned with the fluoroscope to ensure that all interlocking screws have been removed; rotating the nail clockwise will confirm it is free to be removed.
- The impactor is now attached, and the nail can be gently removed either by a combination of clockwise turning and pulling or by use of the slotted mallet. The tube should come out together with the nail.
- At the end of surgery, fluoroscopic images are obtained to verify there isn’t any piece of the cable remaining in the tissue. In rare instances, the remaining piece of cable must be removed by a combination of fluoroscopy and direct vision.
Figure 14. Removal of the single distal interlocking screw can be done percutaneously and similarly to that in the magnetic nail.
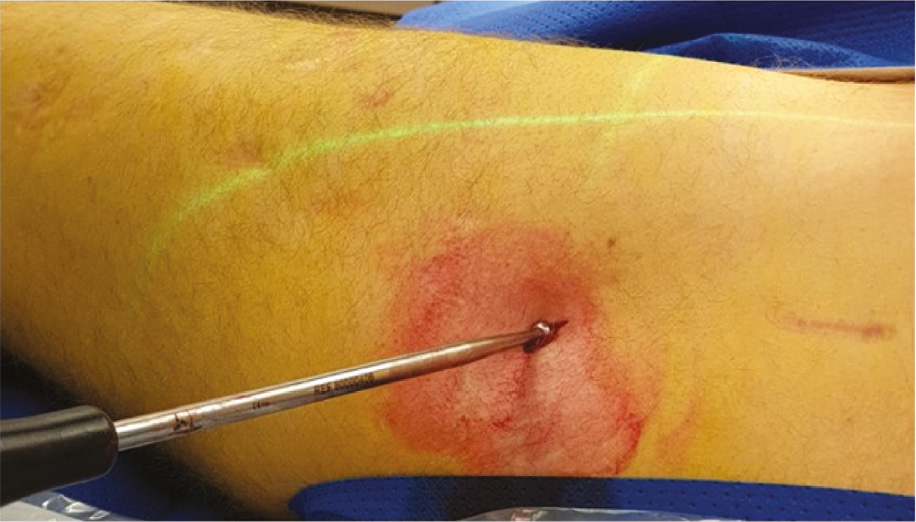
Figure 15. Use the original incision to locate the cable and dissect subcutaneously towards the connector and the receiver. Once the cable is identified, it is cut between the connector and the nail.

Retrograde Intramedullary Lengthening Nail Removal (Precice Magnetic Nail)
- Positioning
The patient is placed in a supine position. A bump is placed under the ipsilateral hip to keep the patella pointing directly anterior. The ipsilateral arm can be positioned at 90 degrees to the torso on an armrest or placed over the chest. Depending on the location of the proximal interlocking screws/pegs, draping to allow access to the entire lower extremity up to the hip may be necessary.
- Removal of the proximal interlocking screws
We have found that there may be bony overgrowth of the proximal interlocking screws in the thin part of the nail. Be sure to rotate the limb until the peg/screw heads are seen in profile to judge whether a percutaneous removal will be possible. If substantial bone has grown around or over the peg/screw heads, then an open removal under direct visualization will be necessary. Key Tip: Occasionally, a small amount of bone can be dislodged from the screw with a percutaneously placed osteotome and careful tapping under image fluoroscopy. Use fluoroscopy to judge whether the same incision for insertion can be utilized again for the removal. Use a straight hemostat to palpate the peg/screw head and clear any tissue from over the peg/screw head. The straight hemostat is easier to use than a curved hemostat because it creates a straight path from the skin to the peg/screw that can be followed by the straight screwdriver handle. The peg/screw head can be captured with the threaded screwdriver for percutaneous removal.
- Capture the distal end of the nail
After the proximal interlocking pegs/screws are removed, the distal end of the nail needs to be captured. Similar to antegrade nail, it is important to capture the nail with the retrieval device prior to removing the distal interlocking pegs/screws. The pegs/screws keep the nail locked in position, so it doesn’t rotate or move while tightening the retrieval device into the distal threads of the nail. A sterile triangle or large towel bump should be used to flex the knee approximately 60 degrees. Key Tip: depending on the patella configuration, such as patella baja, the ideal working angle may be different, and the knee flexion should be adjusted to a smaller bending angle by adding a square pillow under the heel. The goal is to find a straight, continuous line to the nail where the patella is out of the path.
Using the original surgical incision for nail insertion, a standard knee arthrotomy approach is made either through or around the patellar tendon. A guidewire is then inserted into the center of the nail in both the anteroposterior and lateral views under fluoroscopic guidance. Key Tip: For retrograde nail removal, a protective tube/sleeve is needed to prevent damage to the cartilage surfaces of the patella when reaming the bone over the nail. A cannulated reamer is used to remove any bone that may be covering the distal end of the nail. The reamer should be at least 1 mm larger than the diameter of the nail. When removing the reamer, be careful not to pull the guidewire out of the nail. A cannulated nail retrieval device can then be passed over the guidewire and used to capture the threads in the distal part of the nail. Use fluoroscopy to assist lining up the retrieval device perfectly parallel to the nail in both the anteroposterior and lateral views before trying to capture the nail threads.
- Removal of the distal interlocking screws/pegs
Once the nail is captured, the two distal interlocking pegs/screws can be removed through the incision used to insert them. These can typically be removed percutaneously using the threaded peg/screw capture mechanism used to remove the proximal peg/screws. If the surgeon is having difficulty with this technique, then conversion to an open removal can be performed (see antegrade technique). Key Tip: For retrograde nails, blocking screws may have been used; it is preferable to remove the screws prior to nail removal as it decreases the force needed to remove the nail.
- Nail extraction
Once both distal interlocking pegs/screws have been removed, the nail can be carefully extracted either by rotating and pulling the nail or using a slotted mallet. Key Tip: Keep the patella out of the path of the nail to avoid having the nail cause iatrogenic injury to the articular portion of the patella during extraction.
Removal of Retrograde Femur (Fitbone® Motorized Nail)
- After positioning the patient properly (see above Figure 16), the first step of the surgery is to remove the receiver (Figure 17). Typically, the original incision can be used even if the receiver was placed proximally. The receiver cable and the connector are located subcutaneously and dissected proximally under the skin (Figure 18). The cable is cut approximately 3 cm distal to the connector where the cable becomes thin again (Figure 19). Key Tip: Leaving the cable long enough is helpful to allow it to be pulled out through the knee joint later in the procedure (Figure 20). Once identified, the receiver can be pulled out with a Kocher clamp (Figure 21). If the receiver cannot be reached from the original incision site, a separate incision over the receiver can be made. Once identified through the new incision, the cable is cut and the rest of the cable is removed through the original incision as described above.
- The next step is the removal of the pegs/screws. Usually, an incision at the original insertion site can be used. The exact position of the pegs/screws is localized by fluoroscope (Figure 22). Like the magnetic nail, the proximal screw/peg is removed percutaneously by dissecting through the fascia and muscle down to the screw head. The cannulated screwdriver with the threaded cannula can then be used to capture the threads inside the screw head. It is important not to force the threaded cannula into the screw head. Holding the screwdriver at the correct angle to prevent breakage of the threaded cannula in the peg/screw head is also important. The peg/screw is turned counterclockwise while simultaneously pulling the peg/screw out.
- The more distal screws/pegs can be removed in the same manner but at least one peg/screw needs to be left in place to ensure the nail does not move or rotate in the canal when the removal device is attached.
- Once one of the distal screws/pegs is removed, the nail insertion incision is re-opened and a 3.2 mm K-wire is placed through the patella tendon (Figure 23). It is important that the guidewire is aligned perfectly to the center of the nail under fluoroscopy in both the coronal and sagittal planes (Figure 24). The K-wire can be tapped in using a mallet (Figure 25). It is helpful to have the fluoroscope in the AP plane aligned orthogonal to the limb (Figure 26).
- An incision along the K-wire through the patella tendon is performed (Figure 27). The 12 mm cannulated cone is inserted over the K-wire through the patella tendon to the femoral notch (Figures 28 and 29). The hitting device for cone insertion (Figure 30) is used to place the cone’s thick part close to the bone (Figure 31). The 13/12 medium size tube is inserted over the cone through the joint and fixed in place by using a 12 mm hitting device (Figure 32). Tap the hitting device until it sits tight in the bone, but make sure it is not contacting the cable (Figure 33). The hitting device and cone are now removed, leaving the K-wire in place (Figure 34). The tube remains inserted in the bone to ensure clear passage and prevent any debris from passing into the knee joint during nail removal. The 12 mm straight motorized nail reamer is used to open a canal to the nail (Figure 35). The reamer is run until it just begins to contact the cable (Figure 36). The reamer and K-wire are now removed leaving the tube in place.
- Next, the hook is used to catch the cable and pull it out through the tube. Key Tip: There is a hook in the instrument set, but a better one can be created bending a hook at the end of a long 1.8 mm K-wire (Figure 37). The K-wire can be bent into the shape of a hook with pliers. The hook is passed through the tube and pushed into the canal. Rotate the hook 360 degrees and pull it back (Figure 38). It should catch the cable and allow it to be pulled into the cone and then out so it can be visualized. A suture is connected at the end of the cable to pass it through the cannulated retrieval device (Figure 39).
- The retrieval device is now slid over the cable into the nail (Figure 40). It is attached to the nail by the clockwise thread. It is recommended to use the entire thread length until the retrieval device cannot be turned anymore (Figure 41). The impactor can now be attached (Figure 42).
- The last interlocking peg/screw can be removed (Figure 43).
- For retrograde nails, blocking screws are removed prior to nail removal as it decreases the force needed to remove the nail.
- The nail is gently removed either by rotating and pulling it or by using a slotted mallet over the impactor (Figure 44). At this time, it is recommended to hold the tube in place with slight resistance until the nail begins to pull the tube out and both come out together through the patella tendon (Figure 45). This maneuver prevents debris inside of the tube to enter the knee joint (Figure 46).
- After nail removal, fluoroscopic images in both planes should be obtained to ensure the absence of any loose bone or cable fragments (Figure 47).
Figure 16. Position the patient with a towel bump or sterile triangle to allow knee flexion to about 60 degrees.

Figure 17. The original incision can be used to locate the receiver.

Figure 18. The receiver cable and the connector are located subcutaneously and dissected proximally under the skin.

Figure 19. The cable is cut approximately 3 cm distal to the connector where the cable becomes thin again.

Figure 20. Leaving the cable long enough is helpful to allow it to be pulled out through the knee joint later in the procedure.

Figure 21. Once identified, the receiver can be pulled out with a Kocher clamp.

Figure 22. The exact position of the pegs/screws is localized by fluoroscope. The proximal screw/peg is removed percutaneously by dissecting through the fascia and muscle down to the screw head.

Figure 23. Once one of the distal screws/pegs is removed, the nail insertion incision is re-opened and a 3.2 mm K-wire is placed through the patella tendon.

Figure 24. It is important that the guidewire is aligned perfectly to the center of the nail under fluoroscopy in both the coronal and sagittal planes.
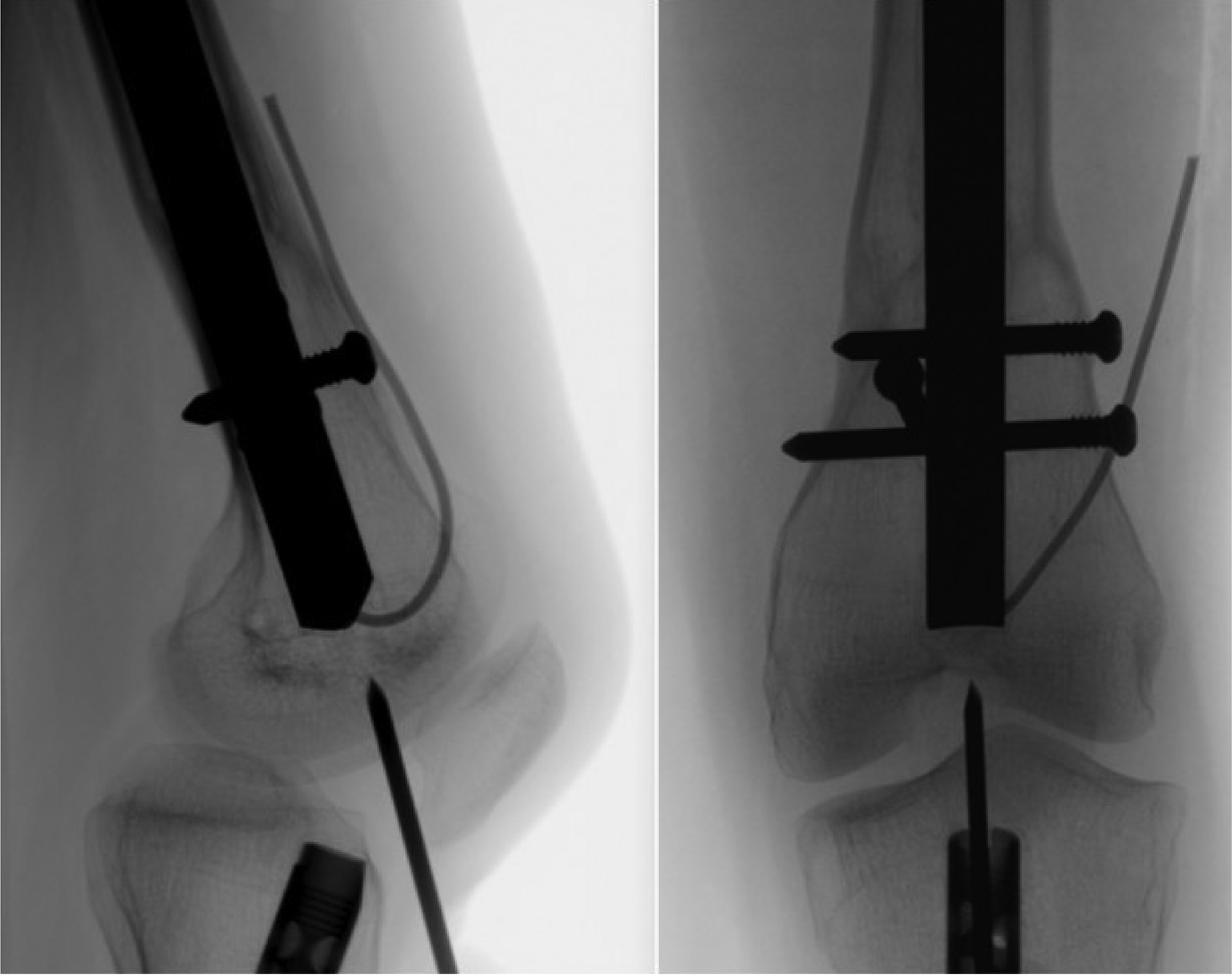
Figure 25. Tap the K-wire into the distal end of the nail with a mallet.
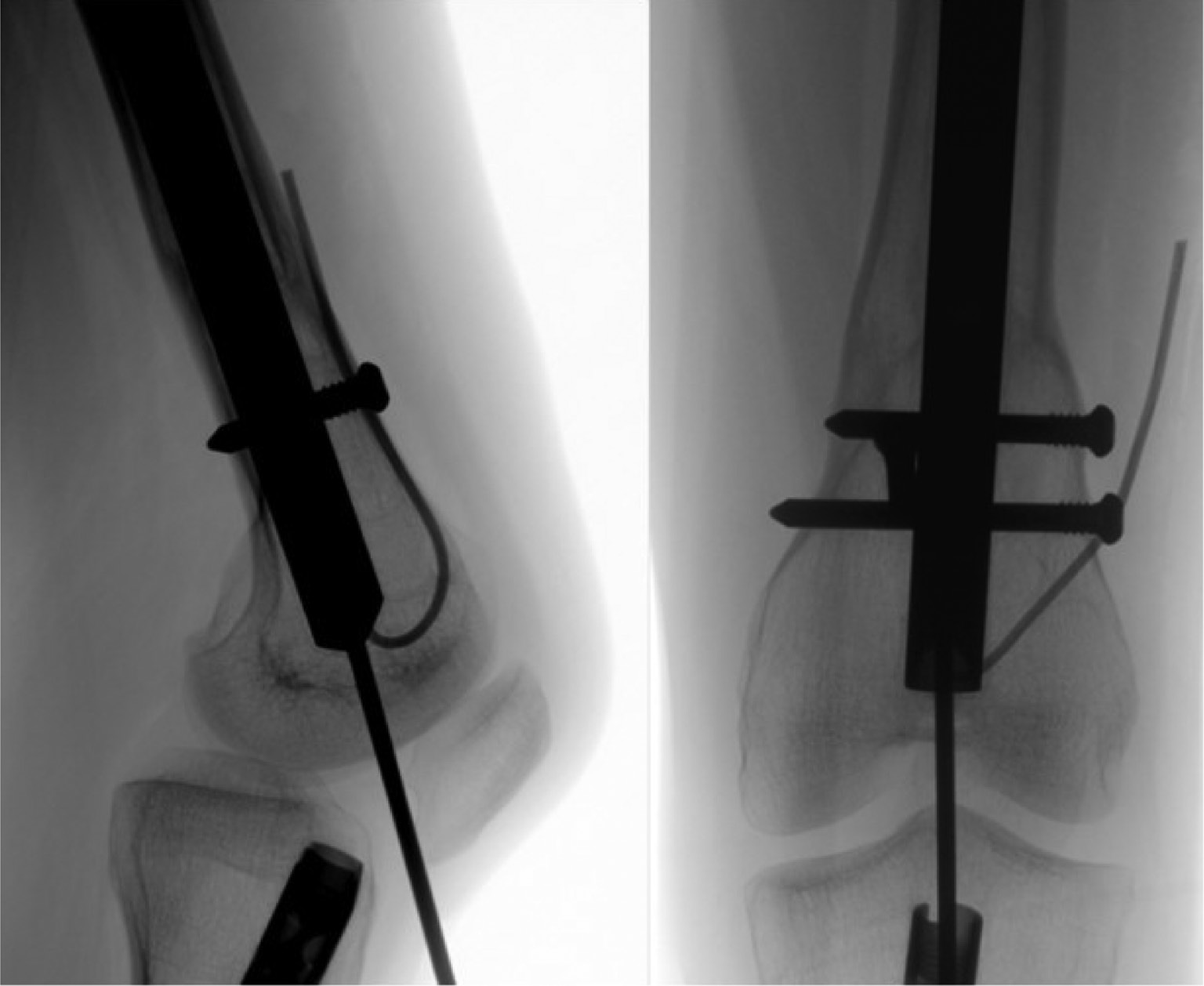
Figure 26. It is helpful to have the fluoroscope oriented perpendicular to the plane of the distal femur.

Figure 27. An incision along the K-wire through the patella tendon is performed.

Figure 28. The 12 mm cannulated cone is placed over the K-wire.

Figure 29. The 12 mm cannulated cone is pushed through the patella tendon to the femoral notch.

Figure 30. The hitting device cone insertion is placed over the wire.

Figure 31. The hitting device for cone insertion is used to place the cone’s thick part close to the bone.

Figure 32. The 13/12 medium-size tube is inserted over the cone through the joint and fixed in place by using a 12 mm hitting device.

Figure 33. Tap the hitting device until it sits tight in the bone, but make sure it is not contacting the cable.
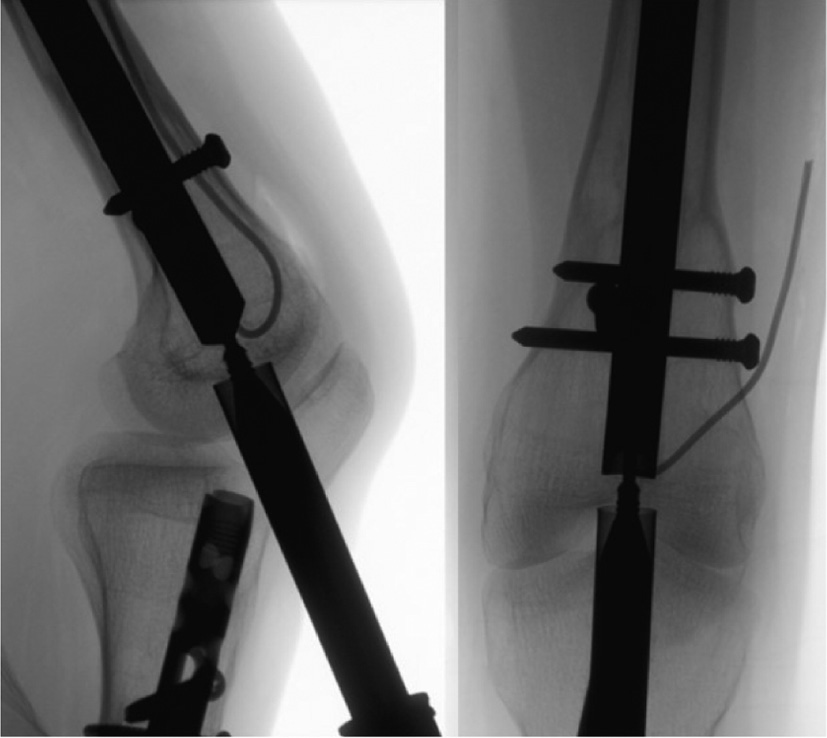
Figure 34. The hitting device and cone are now removed, leaving the K-wire in place.

Figure 35. The 12 mm straight motorized nail reamer is used to open a canal to the nail.

Figure 36. The reamer is run until it just begins to contact the cable.
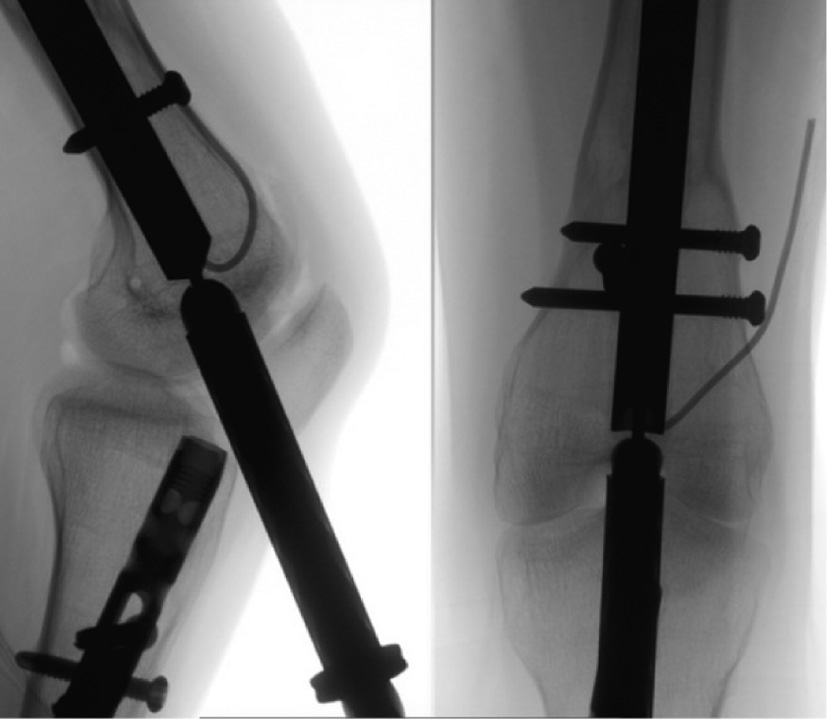
Figure 37. A hook is used to catch the cable and pull it out through the tube. While there is a hook in the instrument set, a better one can be created using a long 1.8 mm K-wire. The K-wire can be bent into the shape of a hook with pliers.
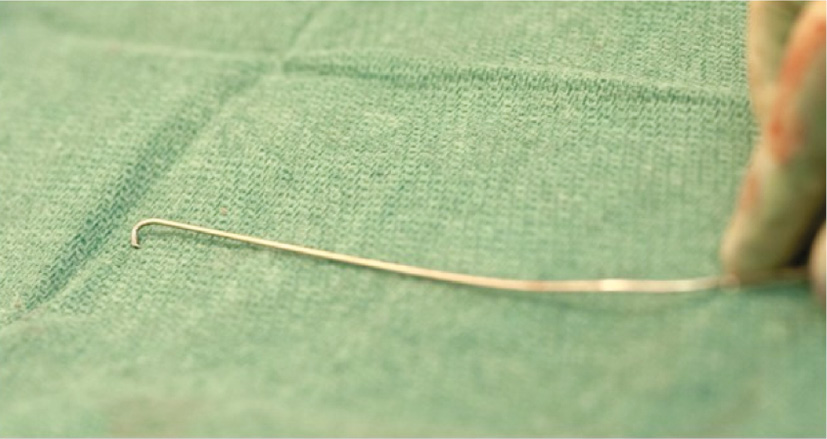
Figure 38. The hook is passed through the tube and pushed into the canal.
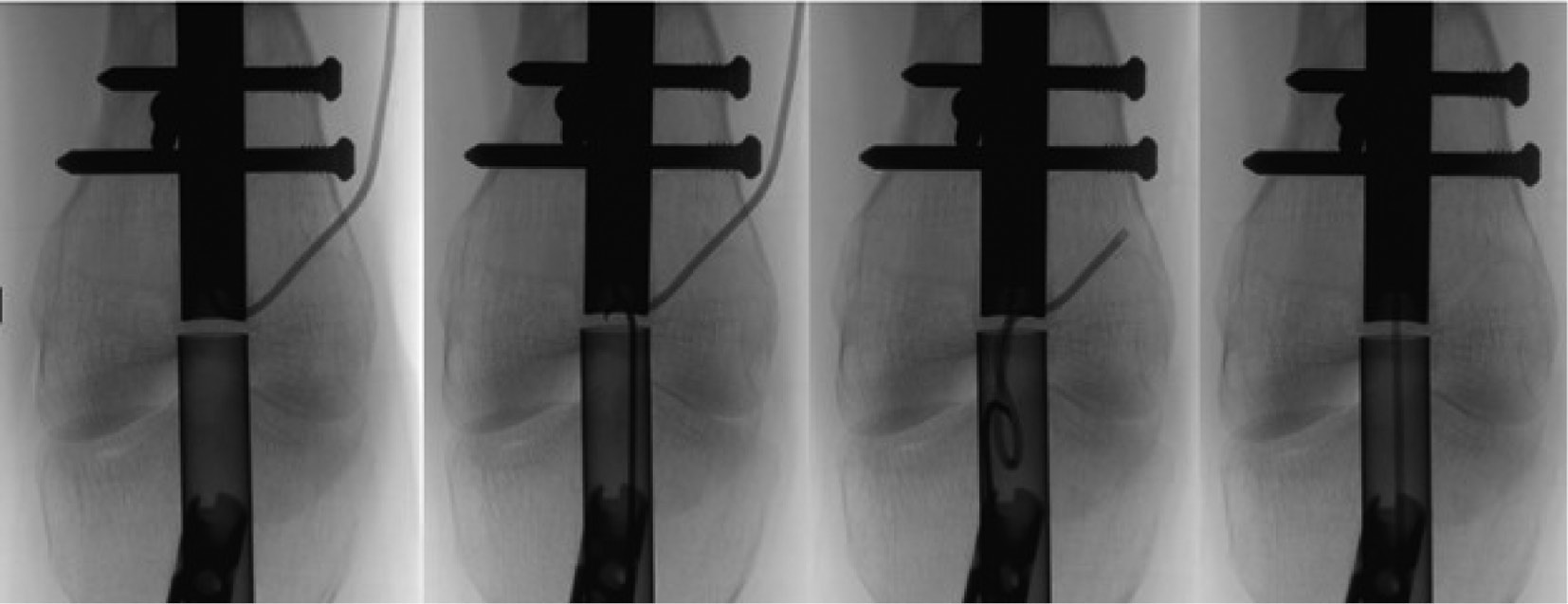
Figure 39. A suture is connected at the end of the cable to pass it through the cannulated retrieval device.

Figure 40. The retrieval device is slid over the cable into the nail.

Figure 41. The retrieval device is attached to the nail by the clockwise thread. It is recommended to use the entire thread until the retrieval device cannot be turned anymore.
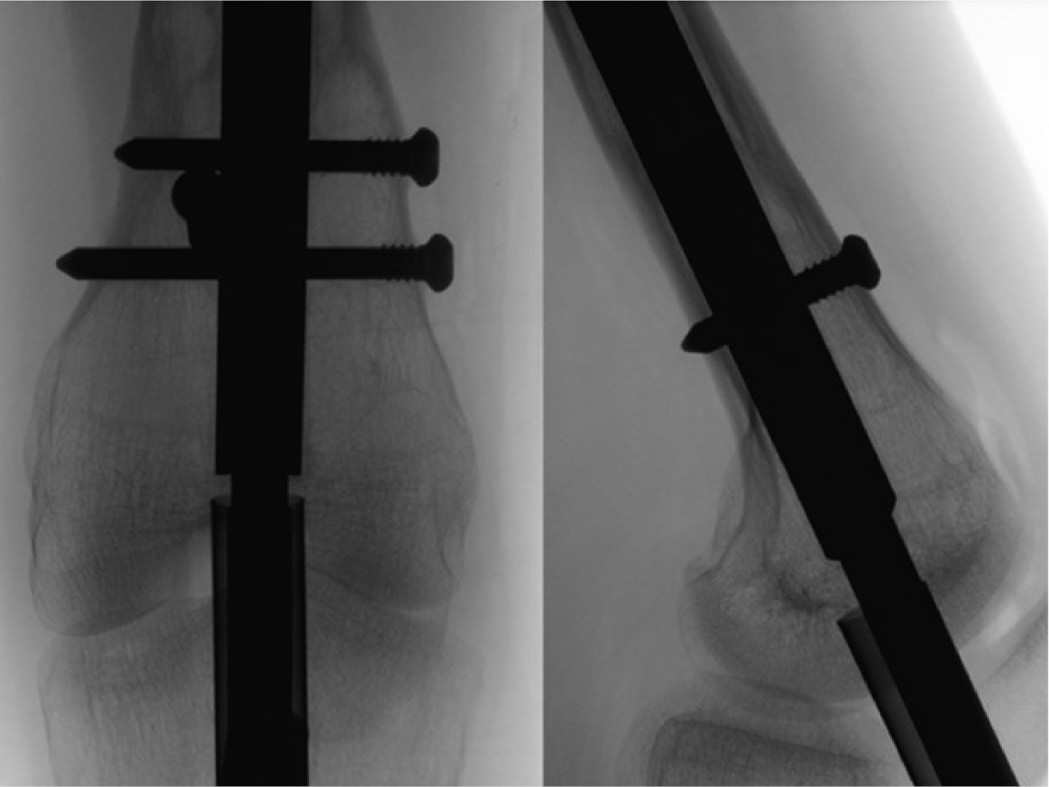
Figure 42. The impactor is attached to the retrieval device.

Figure 43. Remove the last distal interlocking fixation element.

Figure 44. The nail is gently removed either by rotating and pulling it or by using a slotted mallet over the impactor.

Figure 45. It is recommended to hold the tube in place with slight resistance until the nail begins to pull the tube out and both come out together through the patella tendon.

Figure 46. This maneuver prevents debris inside of the tube to enter the knee joint.

Figure 47. After nail removal, fluoroscopic images in both planes should be obtained to ensure the absence of any loose bone or cable fragments.
Summary and Pearls
What if the nail doesn’t want to back out after screw removal?
- Ensure with fluoroscopy that ALL locking screws have been removed.
- Repeat removal of the bone overgrowth at the tip of the nail.
- It can also be helpful to rotate the nail around while pulling it at the same time, as it helps to cut through the bone. The tip of the Fitbone® nail is designed for that reason.
Are endcaps recommended?
Endcaps are available for magnetic nail, and are designed to prevent bony ingrowth into the threaded end portion of the nail (proximal portion of an antegrade nail or distal portion of a retrograde nail) and to protect the integrity of the threads in the end of the nail. They are helpful in situations where an intramedullary implant is designed to be left in place for extended periods of time. While endcaps are available with intramedullary lengthening nail systems, the authors have not found them to be necessary. Since most of these nails are designed to be removed within a year of insertion, bony overgrowth usually is not an issue. Protecting the integrity of the threads is also less important because the cannulated conical nail retrieval devices are designed to aggressively cross thread into the end of the nail. Finally, removing the endcap creates an extra step to the procedure that can be very frustrating, especially if the endcap gets loose in the gluteal soft tissues or the knee joint. The endcaps are not captured like the interlocking screws/pegs so they can fall off the end of the screwdriver during the retrieval process.
On the other hand, endcaps can be helpful if needed for adjusting the nail length. It is possible to add up to an additional 2 cm length with the endcap. This may be necessary in rare cases, such as a bone transport nail, ordering a too short rather than too long nail, or adding length/stability by attaching the longest endcap.
Specific Tips
- When removing a 190 mm length straight universal nail the distal most peg/screw sits so close to the end of the nail that the nail retrieval device can’t be fully attached. Therefore, this nail requires removal of the distal most screw prior to inserting the nail retrieval device.
- For magnetic nail removal, use a tube or sleeve to limit the amount of bone fragments from reaming or nail retrieval contaminating the knee joint. Try to keep all the work done through the path of the sleeve/tube. At the completion of the removal, irrigate the joint copiously prior to closing the incision.
- If the surgeon is planning to replace the lengthening nail with a trauma nail to protect the regenerate bone, remember that the lengthening nail is no longer its original length. The lengthening of the bone/nail needs to be considered when choosing the appropriate length of the trauma nail to span the new femur length. Be aware that most trauma nails are not straight and have a different curvature than the lengthening nails. This might result in increased resistance and stress on the bone when exchanging with a trauma nail. In such cases, either the canal must be enlarged by further reaming or a smaller diameter trauma nail must be inserted.
Disclaimer
C. Iobst: Consultant for NuVasive, Smith and Nephew, Orthofix, and Wishbone Medical; S. Kold: Consultant for Wishbone Medical; M. Mikužis: No conflicts of interest to disclose.