
Current Concept Review
Biomechanical Basis for Treatment of Pediatric Foot Deformities Part I: Mechanics of the Foot
1Bloomberg Children’s Center, Johns Hopkins Hospital, Kennedy Krieger Institute, Baltimore, MD; 2Department of Pediatric Orthopedics, Massachusetts General Hospital, Boston, MA; 3Department of Paediatric Orthopaedics, Kasturba Medical College, Manipal, India
Correspondence: Benjamin Joseph, MCh Orth, FRCS Ed, 18 HIG, HUDCO Colony, Manipal, 576104, Karnataka, India. E-mail: [email protected]
Received: March 15, 2022; Accepted: March 20, 2022; Published: May 1, 2022
DOI: 10.55275/JPOSNA-2022-0028
Volume 4, Number 2, May 2022
Abstract:
The foot functions as a flexible structure during the initial part of stance phase but changes into a rigid structure in the terminal part of stance to enable a powerful push-off. This illustrated review describes the normal mechanics of the foot during inversion and eversion and explains in some detail how the calcaneum moves under a stationary talus in three planes simultaneously around a single oblique axis. During eversion, the calcaneum dorsiflexes, abducts, and pronates while it plantarflexes, adducts, and supinates during inversion. The talus remains static while the rest of the foot moves as a unit, referred to as the calcaneo-pedal unit (CPU), around the head of the talus. The socket-like hollow in the CPU consisting of the anterior and middle articular facets of the calcaneum, the articular fact of the navicular and the spring ligament constitute the “acetabulum pedis” which rotates around the talus. On occasion, the foot functions like a twisted plate influencing the inter-relationship between the hindfoot and forefoot as a forefoot deformity may cause a secondary compensatory deformity of the hindfoot. Understanding normal foot mechanics will facilitate greater understanding of altered mechanics seen in abnormal foot deformities.
Key Concepts:
- The foot is divided into the hindfoot and forefoot; the mechanics of movement of the joints of the forefoot and hindfoot are distinctly different.
- The subtalar joint moves around a uniquely oriented oblique axis which permits movement of the calcaneum under a static talus in three planes and these movements occur simultaneously.
- The foot behaves like a twisted plate such that primary deformities of the forefoot can cause secondary deformities in the hindfoot with concomitant elevation or depression of the longitudinal arch of the foot.
The human foot is one of nature’s works of art and, as such, it has not been fully recognized and explained. It will require a deal of scientific investigation before this structure is fully understood.
—Georg Hohmann
Introduction
The foot is a complex structure comprising of several bones articulating through joints that have separate axes of movement which permit varying degrees of freedom of movement. The foot can be divided into the hindfoot, mid-foot, and forefoot (Figure 1A) for the convenience of description. However, it is important to be aware that these parts of the foot work in unison and a deformity or dysfunction of one region of the foot affects the rest of the foot. The foot can also be divided into two functional columns: a medial column and a lateral column (Figure 1B).
Figure 1. (A) The foot consists of the hindfoot in red (talus & calcaneum), the mid-foot in green (navicular, cuboid, and cuneiforms), and the forefoot in white (metatarsals & phalanges). (B) The foot may be considered to function as two columns: a medial column (red) and a lateral column (blue).

The foot functions as a flexible structure which absorbs force during the initial part of the stance phase of the gait cycle but changes into a rigid structure in the terminal part of the stance to enable a powerful push-off.
The Hindfoot
Anatomy
The bones of the hindfoot are the talus and the calcaneum. Although the subtalar joint is the only joint truly in the hindfoot, the ankle, or talo-crural joint, also needs to be considered as part of the hindfoot because most deformities of the hindfoot involve both the ankle and the subtalar joints.
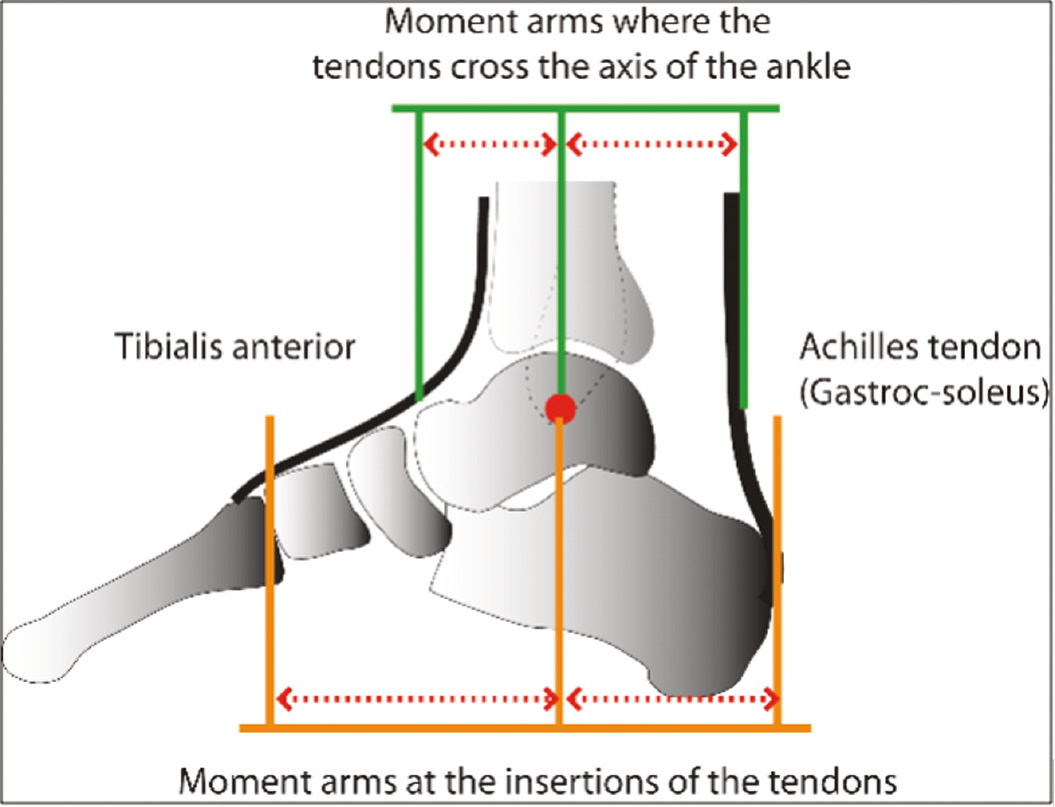
The ankle joint is a synovial joint between the talus and the tibia and fibula where dorsiflexion and plantarflexion occur around an axis passing through the medial and lateral malleoli. The movement of the talus is not brought about by any muscle acting directly on the talus, as no muscle inserts into the talus. Rather, the talus moves in response to contraction of muscles that insert distal to it. The primary plantarflexor of the ankle is the powerful gastrocnemius-soleus muscle that inserts into the tuberosity of the calcaneum, while the primary dorsiflexor of the ankle is the tibialis anterior that inserts into the medial cuneiform and the base of the first metatarsal.
The tendons of these muscles cross the axis of the ankle at some distance from the axis and similarly the insertion of both these muscles are even further from the axis of movement of the ankle (Figure 2). The force moments generated by these muscles are dependent on the length of their lever arms and any reduction in the length of these lever arms will appreciably reduce their power. Inversion and eversion of the foot occurs at the talo-calcaneal or subtalar joint; these movements facilitate the foot to adapt to uneven terrain. During inversion and eversion, the talus does not move, but the calcaneum and the rest of the foot moves around the head of the talus.
Figure 2. Moment arms of the tibialis anterior and the Achilles tendon in relation to the axis of the ankle joint (red dot).
Mechanics of the Ankle and Subtalar Joints
An early nineteenth century work of art by William Henry Hunt*, an English artist (Figure 3), draws our attention to a cart and a boat, and in the context of this review, we can draw comparisons to the human ankle and subtalar joints. The cart wheel moves around a transverse axis permitting one degree of freedom; it can rotate forward or backward. Similarly, the ankle joint functions around a bi-malleolar axis with one degree of freedom of movement permitting dorsiflexion and plantarflexion. These movements are integral parts of normal gait and they occur at very specific points in the gait cycle. Though the range of dorsiflexion and plantarflexion during normal walking is modest, abolition of either of these movements will result in a limp.
Figure 3. Untitled sketch by William Henry Hunt (Photo © Tate, London, 2022 - Image released under Creative Commons CC-BY-NC-ND (3.0 Unported).

The mechanics of the subtalar joint are unique and have been the subject of several studies.1–5 Kapandji, in his superbly illustrated books, The Physiology of Joints, credited Farabeuf* with comparing movement of the calcaneum during inversion and eversion to movement of a boat on the waves.6 A boat has three degrees of freedom of rotational movement around three independent axes of movement that are at right angles to each other enabling the boat to roll, yaw, and pitch as it moves on the waves (Figure 4).
Figure 4. Diagrammatic representation of movement of a boat around three separate axes.

In comparison, the calcaneum moves under the talus during inversion and eversion in three planes: the calcaneum abducts (akin to yawing of a boat), it dorsiflexes (akin to pitching of a boat), and it pronates (akin to rolling of a boat) during eversion and adducts, plantarflexes and supinates during inversion. However, there are two cardinal differences between the movement of a boat on the waves and movement of the calcaneum during inversion and eversion. Firstly, the calcaneum moves around a single axis that permits tri-planar movement. Secondly, since these three movements of the calcaneum occur around a single axis, all three movements occur simultaneously and cannot occur independently.
The Axis of the Subtalar Joint
Henke and Manter are credited with deducing that the tri-planar axis of the subtalar joint is oblique, running downward, posteriorly (at an angle of around 45 degrees to the horizontal and 16 degrees laterally).3,4 Other studies have suggested angles slightly higher or lower than these and more recent work suggests that this axis is not fixed and may move a few degrees as the foot moves.5 However, for all practical purposes the axis may be considered to be at 45 degrees to the horizontal running from the dorsal aspect of the neck of the talus, through the sinus tarsi through the substance of the interosseous talocalcaneal ligament and exiting at the lateral part of the calcaneal tuberosity.
An articulated functional model of the hind foot made by Aloysio Campas da Paz in 1978,7 was replicated here. The talus was fixed rigidly while the calcaneum was free to move around the axis (a stout wire passed in the direction of the true axis of the subtalar joint (Figure 5A).
Figure 5. Articulated model of the hindfoot that can simulate movement of the subtalar joint. The talus is held rigidly, but the calcaneum is free to move under the talus around the subtalar axis (A). When viewed from the front in the inverted position, the anterior end of the calcaneum is under the talar head, and the talar and calcaneal wires are very close to each other (B). In the everted position, the anterior end of the calcaneum has moved laterally (abducted) and is no longer under the talar head, and the talar and calcaneal wires are diverging (C). When viewed from the lateral aspect in the inverted position, the sinus tarsi is open (D), the sinus tarsi closes, and the calcaneum dorsiflexes as the hind foot everts (E). The pronation of the calcaneum during eversion is evident when the model is viewed from the back (F, G). The original position of the calcaneum in inversion is shown in dotted red tracings superimposed on the respective everted positions.

Two additional wires were inserted: one in the long axis of the talus and one in the long axis of the calcaneum. The model was viewed from the front as the calcaneum was moved from full inversion (B) to eversion (C). During eversion, the calcaneum abducts with its anterior end (the cuboid surface) moving laterally and the talar and calcaneal wires diverging. When viewed from the lateral aspect, the sinus tarsi which is widely open in inversion (D) closes as the calcaneum adopts the everted position and simultaneously, the calcaneum dorsiflexes (E). When viewed from the back, the calcaneum pronates in eversion (F, G).
The mechanics of subtalar movement can be appreciated better by observing the movement of the calcaneum on the functional model of the hindfoot of Aloysio Campas da Paz (see accompanying presentation—Understanding the Mechanics of Subtalar Movement).
The Acetabulum Pedis
Of late, there has been a trend to revive a concept initially outlined by Scarpa* related to the mechanics of hindfoot motion.8–12 He likened the movement of the head of the talus to that of the femoral head in the hip joint and suggested that the structures that the talar head articulated with was a cup-like “socket” and coined the term “acetabulum pedis” for this socket (Figure 6).
Figure 6. Diagrammatic representation of the acetabulum pedis. The upper surface of the calcaneum is shown after removal of the talus (top left). The head of the talus articulates with the acetabulum pedis (top right and bottom).

The acetabulum pedis includes the articular surfaces of the anterior and middle facets of the calcaneum, the concave articular surface of the navicular bone and the plantar calcaneo-navicular ligament or the spring ligament that stretches across the gap between the articular surfaces of the navicular and the calcaneum (Figure 6).
The Calcaneo-pedal Unit
When the normal foot inverts or inverts, the talus remains static and the rest of the foot (i.e., the calcaneum, cuboid, navicular, cuneiforms and the metatarsals) referred to as the calcaneopedal unit, or CPU, moves en bloc around the talus (Figure 7).
Figure 7. The calcaneo-pedal unit (blue) rotates around the static talar head (i.e., the acetabulum pedis moves around the talar head).

The unified movement of the CPU is facilitated by strong ligaments which bind the tarsals to each other and to the metatarsals. In addition, the unique insertion of the tibialis posterior with slips to all the tarsal bones with the exception of the talus also ensures that all the tarsals move in unison when the muscle contracts.
The Mid-Tarsal Joint
The mid-tarsal joint is the joint between the hindfoot and the mid-foot and consists of two distinct joints: the talo-navicular and the calcaneo-cuboid joint. The talo-navicular joint is more appropriately referred to as the talo-calcaneo-navicular joint as the talo-navicular articulation is part of the larger articulation between the acetabulum pedis and the CPU. The talo-navicular part of the mid-tarsal joint is far more mobile than the calcaneo-cuboid joint. As a consequence, the medial column of the foot is more mobile than the lateral column. There is no consensus about the axis of the mid-tarsal joint with some investigators suggesting that midtarsal movement occurs around two separate axes (a longitudinal axis and an oblique axis) while others suggest that tri-planar motion occurs around a single axis.13
The muscles acting on the mid-tarsal joint are primarily the invertors and evertors of the foot. While the tibialis posterior inserts into the tuberosity of the navicular with slips to all the tarsal bones barring the talus, the peronei longus and brevis insert into the bases of the first and fifth metatarsals, respectively. These muscles are responsible for supination and pronation of the forefoot.
The Mid-Foot
The mid-foot consists of the navicular, cuboid, and the three cuneiform bones. Very little movement occurs between these bones.
Relationship Between Hindfoot and Forefoot Motion
Reciprocal Movement Between the Hindfoot and Forefoot
Though the forefoot usually moves as an integral part of the CPU when the hind foot moves, there are situations when the movement of the hindfoot and forefoot are in opposite directions. This is seen when forefoot deformities prevent the forefoot from resting flat on the ground. When there is a supination deformity of the forefoot, only the lateral border of the forefoot rests on the ground; the forefoot is made plantigrade by compensatory eversion of the hindfoot which adopts a valgus position. Conversely, when there is a pronation deformity of the forefoot with the medial border of the foot resting on the ground, compensatory hindfoot varus develops to make the forefoot plantigrade (Figure 8).
Figure 8. Deformities of the forefoot can create compensatory deformities in the hindfoot. The reciprocal movement of the hindfoot in response to a forefoot deformity is brought about by the foot functioning like a twisted plate.

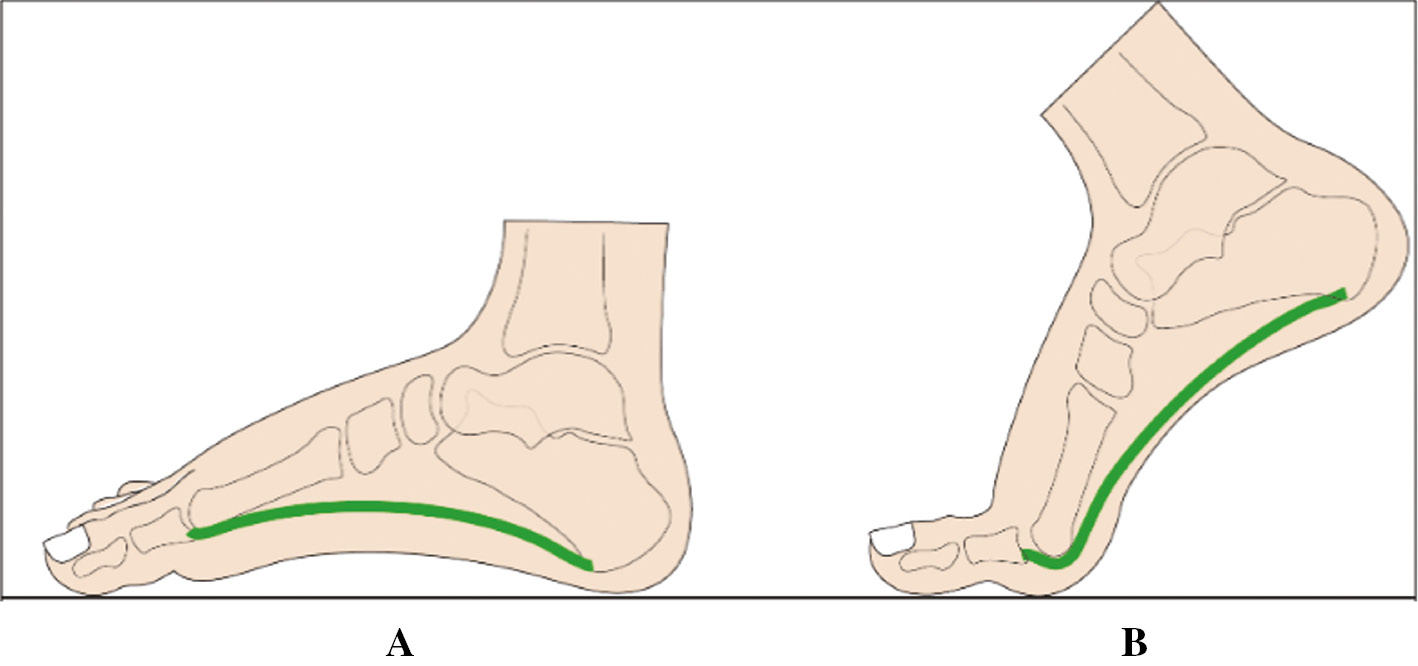
The foot, in these situations, behaves like a twisted plate that untwists when the hindfoot moves into valgus with reduction of the height of the medial longitudinal arch and which twists more when the hindfoot moves into varus with accentuation of the arch (Figure 8). An example of this phenomenon is illustrated in Figure 9.
Figure 9. The fore foot is pronated due to a plantarflexed first ray secondary to paralysis of the tibialis anterior (A). On weight-bearing, the compensatory hindfoot varus enables the forefoot to rest on the ground with accentuation of the medial arch (B).

Effect of Hind Foot Position on Forefoot Motion
The flexibility of the forefoot varies with the position of the hindfoot. The range of dorsiflexion and plantarflexion of the metatarsals is significantly greater when the hindfoot is inverted while very little dorsiflexion and plantarflexion of the metatarsals is possible when the hindfoot is everted.14
The Medial Longitudinal Arch
There are three arches of the foot, the medial and lateral longitudinal arches and the transverse arch. The arched structure of the foot facilitates shock absorption. The medial longitudinal arch is the most important of the three arches and its integrity is dependent on intrinsic and extrinsic mechanisms that support the arch and prevent it from collapsing when loaded (as in standing, walking, or running and jumping). The intrinsic mechanisms include inter-osseus ligaments between each adjacent bones which constitute the arch, ligaments which span more than two bones and the plantar fascia (aponeurosis). The plantar fascia spans the full length of the arch from the calcaneum to the toes. Dorsiflexion of the toes results in tightening of the plantar fascia with accentuation of the arch (Figure 10). The extrinsic mechanisms that support the arch are muscles that sling up the arch and the tibialis posterior is the most important muscle responsible for the integrity of the arch.
Figure 10. The effect of dorsiflexion of the great toe on the plantar fascia.
Pathomechanics of Foot Deformities in Children
Features of Common Pediatric Foot Deformities
Foot deformities in children may develop as a result of
- contractures of tendons, joint capsules and ligaments.
- laxity of tendons, joint capsules and ligaments.
- muscle imbalance across joints due to weakness or spasticity of one group of muscles.
The consequences of these soft tissue abnormalities may include:
- Abnormal alignment of the talus
- Subluxation or dislocation of the talo-navicular joint
- Alterations in the configuration of the medial longitudinal arch
- Lever arm dysfunction
In the following section (Part II), the pathomechanics of pes planus, congenital vertical talus, pes cavus, and deformities secondary to neuromuscular disorders will be discussed.
Disclaimer
No funding was received by the authors. The authors have no conflicts of interest to disclose.
*Footnotes
Hunt, who was born in 1790, had deformed legs that impeded his mobility. Exact details of his physical impairment are not available. He convinced his father to permit him to pursue a career in art, a decision that did not find favor with an uncle who is supposed to have said, “he was always a poor cripple, and he was fit for nothing, they made an artist out of him.” Hunt became an accomplished artist and received sufficient recognition to be admitted to the Royal Academy.
Louis Hubert Farabeuf (1841-1910) is regarded as a pioneer of topographic, clinical and applied surgical anatomy. Above all, he was a devoted teacher of anatomy.
Antonio Scarpa (1752-1832) was Professor of Anatomy and Surgery at the University of Pavia in Italy. Scarpa became an honorary member of the Royal Society of London in 1791 and of the Royal Swedish Academy of Sciences in 1821. He was a skilled general surgeon as well as being proficient in eye, ear, and orthopaedic surgery.
References
- Huson A. Biomechanics of the tarsal mechanism. A key to the function of the normal human foot. J Am Podiatr Med Assoc. 2000 Jan;90(1):12–17.
- Lapidus PW. Kinesiology and mechanical anatomy of the tarsal joints. Clin Orthop Relat Res. 1963;30:20-36.
- Hicks JH. The mechanics of the foot. I. The joints. J Anat. 1953 Oct;87(4):345–357.
- Elftman H, Manter JT. The axis of the human foot. Science. 1934 Nov 23;80(2082):484.
- Kirby KA. Subtalar joint axis location and rotational equilibrium theory of foot function. J Am Podiatr Med Assoc. 2001 Oct;91(9):465-487.
- Kapandji IA. The Physiology of Joints 1st Ed Vol 2. Edinburgh: E & S Livingstone; 1970:154-194.
- da Paz AC Jr, de Souza V. Talipes equinovarus: pathomechanical basis of treatment. Orthop Clin North Am. 1978 Jan;9(1):171-185.
- Mosca VS. Clubfoot pathoanatomy - biomechanics of deformity correction: a narrative review. Ann Transl Med. 2021 Jul;9(13):1096.
- Ghanem I, Massaad A, Assi A, et al. Understanding the foot’s functional anatomy in physiological and pathological conditions: the calcaneopedal unit concept. J Child Orthop. 2019 Apr 1;13(2):134-146.
- Epeldegui T, Delgado E. Acetabulum pedis. Part I: Talocalcaneonavicular joint socket in normal foot. J Pediatr Orthop B. 1995;4(1):1-10.
- Epeldegui T, Delgado E. Acetabulum pedis. Part II: Talocalcaneonavicular joint socket in clubfoot. J Pediatr Orthop B. 1995;4(1):11-16.
- Ledoux WR, Sangeorzan BJ. Clinical biomechanics of the peritalar joint. Foot Ankle Clin. 2004 Dec;9(4):663-683.
- Tweed JL, Campbell JA, Thompson RJ, et al. The function of the midtarsal joint: a review of the literature. Foot (Edinb). 2008 Jun;18(2):106-112.
- Blackwood CB, Yuen TJ, Sangeorzan BJ, et al. The midtarsal joint locking mechanism. Foot Ankle Int. 2005 Dec;26(12):1074-1080.