
Master’s Surgical Techniques
Percutaneous Anterior Distal Femoral Hemiepiphysiodesis Using Simultaneous Biplanar Fluoroscopy
1Department of Orthopedic Surgery, Mayo Clinic, Rochester, MN; 2Department of Orthopaedic Surgery, University of Minnesota, Minneapolis, MN; 3Gillette Children’s Specialty Healthcare, St. Paul, MN
Correspondence: Andrew G. Georgiadis, MD, Gillette Children’s Specialty Healthcare, 200 University Ave. E, St. Paul, MN. E-mail: [email protected]
Received: March 28, 2022; Accepted: June 10, 2022; Published: August 1, 2022
DOI: 10.55275/JPOSNA-2022-0077
Volume 4, Number 3, August 2022
Abstract:
Knee flexion contracture is a common target for surgical treatment in children with cerebral palsy. Anterior distal femoral hemiepiphysiodesis (ADFH) with percutaneous screws is an alternative technique to tension-band plate and screw constructs. The technique can be demanding and correct screw placement is highly reliant on accurate intraoperative imaging. We describe a technique for ADFH using percutaneous cannulated screws with utilization of simultaneous biplanar fluoroscopy to facilitate efficient and accurate screw placement. The indications, technique, postoperative treatment, and pitfalls of this procedure are reviewed.
Key Concepts:
- Knee flexion contracture can be treated effectively with anterior distal femoral hemiepiphysiodesis using percutaneous screws.
- Percutaneous screw technique for ADFH can be safely and efficiently expedited with simultaneous biplanar fluoroscopy.
- Careful attention to room setup, patient and surgeon positioning, and several key intraoperative steps can facilitate the screw ADFH technique.
Introduction
Knee flexion contractures and a crouch gait pattern are common clinical problems in the growing child with cerebral palsy and other neuromuscular conditions. Treatment of small contractures with hamstring lengthening is commonly performed but may lead to decreased hip extensor power generation and increased anterior pelvic tilt.1 Recurrence is common, and hamstring lengthening can be repeated, but with less predictable results.1 Anterior distal femoral hemiepiphysiodesis (ADFH) has been described using staples or plate and screw constructs.2–4 Correction of the deformity with these methods has been reliable, but staple migration is a reported complication, and knee pain is frequently reported with plate and screws, possibly related to intra-articular implant bulk. Recently, percutaneous screw only techniques have been described with reliable deformity correction and less risk of complications or postoperative pain.4,5
Percutaneous ADFH is an effective procedure but is highly reliant on accurate intraoperative imaging and is demanding because of screw trajectory and thigh geometry.6 The purpose of this manuscript is to describe the step-by-step technique for ADFH using percutaneous cannulated screws with the utilization of two C-arm devices to facilitate efficient and accurate screw placement. The indications, technique, postoperative treatment, and pitfalls of this procedure are reviewed.
Description of the Method
Indications
Guided growth of the anterior distal femur can be used to correct fixed knee contracture deformity in children with cerebral palsy at any Gross Motor Function Classification System level as well as other conditions. It must be performed prior to skeletal maturity with at least 1-2 years of growth remaining with more growth required for more severe contracture correction. In our hands, this procedure is typically limited to correction of flexion contractures less than 20 degrees and correction of >50% of the contracture magnitude is more likely to occur after ADFH if a child is under 11 years of age at the time of surgery.7
Positioning
The patient is positioned supine on a radiolucent table. A tourniquet may be used but is not necessary, as minimal blood loss occurs with this percutaneous technique. Limiting towels, tourniquets, tubing, or excessive drapes between the legs avoids impingement on the instrumentation, particularly for the medial-sided screws. The feet are brought near the end of the operating table (Figure 1).
Figure 1. Illustrative schematic demonstrating C-arm positioning relative to the patient’s right knee. The knee is flexed about 30–45 degrees on a bolster, and both fluoroscopy units are rotated to obtain the appropriate orthogonal images without impingement on one another. (Copyright © Andrew G. Georgiadis, MD.)

Operative Technique
If performing bilateral procedures, knees are addressed sequentially. The knee is elevated on a sterile bump and sloped about 30–45 degrees cephalad from hip to knee to avoid radiographic interference with the contralateral extremity. The first C-arm is positioned perpendicular to the operating table in the lateral position with the arm beneath the table leaning toward the patient’s head (Figure 2). Since the end of the medial femoral condyle is typically distal to the end of the lateral femoral condyle in a femur without coronal plane deformity, the leg is typically slightly adducted towards the midline to facilitate optimal x-ray visualization. Once the lateral x-ray demonstrates overlapping femoral condyles, the extremity is held in place and the second C-arm is brought in from the foot of the bed and arched over the knee to obtain an AP image of the distal femur. Typically, the C-arm for the lateral images must be rotated toward the head of the bed to avoid impingement with the lower aspect of the second C-arm (Figure 2). Once the C-arms are positioned, an assistant holds the knee in place for the remainder of the procedure to preclude any need for adjustments in C-arm positioning.
Figure 2. Photographs demonstrating the dual C-arm device arrangement after full prep and drape. The lateral C-arm is rotated to make room for the base of the anteroposterior C-arm, which approaches the patient from the foot of the bed. In the image above, the right knee is flexed, and the surgeon can be positioned near the patient’s chest on the ipsilateral side. Careful planning of viewing screens can maximize efficiency and surgical flow.

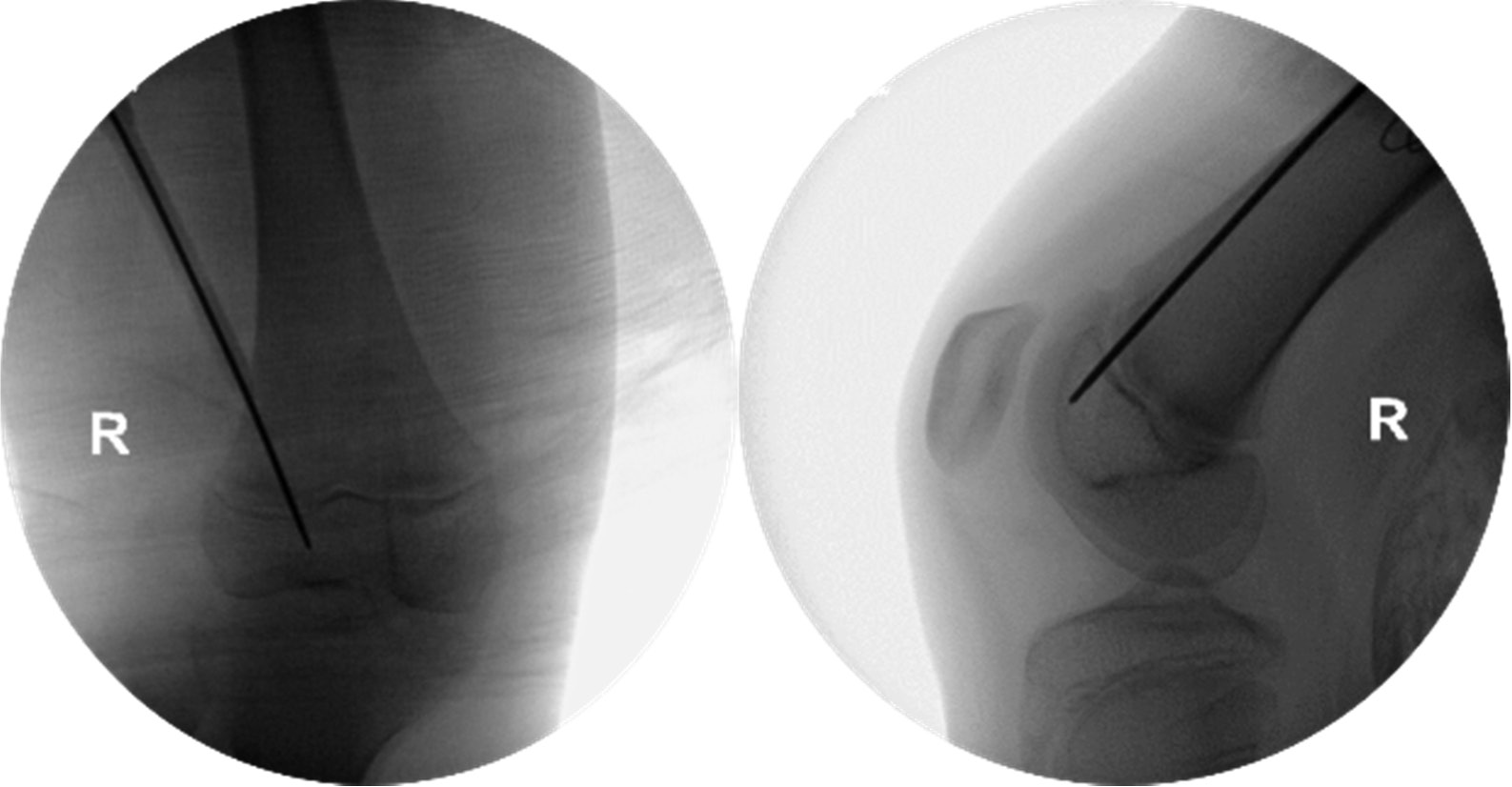
A radiopaque instrument placed in the intended guidewire trajectory is used to guide the incision location. A 5-10 mm incision is made through the skin. A guidewire is inserted onto the lateral femoral metaphysis about 2 cm proximal to the physis on the AP view. A lateral image guides the insertion point to be in the anterior third of the femoral metaphysis. Once the starting point is obtained, the wire driver is brought toward the limb to direct the guidewire as longitudinally as possible in the coronal plane. This can be facilitated by using a thin cardboard barrier between the skin and guidewire or by using a wet sponge to press the guidewire against the lateral thigh to prevent thermal skin injury as recommended by Dr. Robert Kay (pers. commun.). When the trajectory is appropriate on both images, the guidewire is advanced across the physis into the epiphysis. Guidewire placement should be across the anterior third of the physis. The lateral x-ray guides the final depth of the guidewire as the tip of the guidewire should be proximal to the articular surface (Figure 3).
Figure 3. Anteroposterior and lateral fluoroscopic images demonstrating initial guidewire placement in the anterior third of the lateral distal femoral physis.
A depth gauge is used over the wire and inserted down to the cortex. A screw is selected that is 2-4 mm longer than measured to facilitate future screw removal and avoid bone overgrowth. A cannulated drill can be used to open the cortex over the guidewire but is not required given the soft metaphyseal bone. The authors typically use 4.5 mm fully threaded cannulated screws for fixation. The screw is inserted under fluoroscopic guidance on the lateral image to avoid inadvertent joint penetration with final seating.
The same technique is repeated for the medial side. Typically, the medial incision is a few centimeters proximal to the lateral incision to account for a thicker medial soft-tissue envelope. This allows for a more vertical trajectory. The starting point is again in the anterior third of the femoral metaphysis and approximately 2-3 cm proximal to the physis. Final x-rays demonstrate appropriate positioning (Figure 4).
Figure 4. Anteroposterior and lateral fluoroscopic images demonstrating final screw position.

Tips and Pearls
The procedure can be quick and efficient with the use of dual C-arms. If the limb is held in the same position throughout, the entire procedure can be completed without any further adjustment of positioning for any view. In our experience, a single screw can be placed in less than 5 minutes or an entire limb in less than 10 minutes.
Given the soft-tissue constraints, especially on the medial side of the thigh, the most common error is guidewire placement that is too oblique in the coronal plane. This results in the tip of the screw underlying the trochlea and increasing the risk of joint penetration and providing minimal epiphyseal purchase to guide growth. Gently bending the guidewire on insertion, with slow use of the wire driver, without permanent deformation, helps achieve a longitudinal trajectory. Avoiding excessive draping in the groin area limits interference with the wire driver as the guidewire is advanced. This is especially important in patients of short stature.
Placing screws that are about 4 mm longer than measured has facilitated easier future removal without symptomatic hardware prominence. Complete seating of the screw head to the bone surface is not necessary to achieve the intended osseous correction.
Postoperative Care
The patient is allowed full-weightbearing immediately. The procedure is typically performed on an outpatient basis if not combined with other more invasive procedures. Serial AP and full-extension lateral knee x-rays are obtained typically at 3-month intervals to monitor the deformity correction. The screws are removed once full correction or slight overcorrection is obtained.
Comparison to Other Methods
In 2020, Nazareth et al. performed a comparative study examining three different techniques for ADFH, including a plate and screw construct, as well as single and double percutaneous screw techniques.4 They found a significant reduction in knee flexion contracture in all three groups and no difference among the techniques. Postoperative knee pain was significantly more prevalent in the plate and screw construct than with either of the percutaneous screw techniques.
Percutaneous techniques are technically challenging because precise screw placement is essential to obtain deformity correction and avoid joint penetration. Accurate intraoperative fluoroscopy is critical to a successful operation. Since adopting this technique, the authors have found that obtaining simultaneous orthogonal images expedites guidewire insertion and can reduce radiation exposure to the patient, surgeon, and operating room staff, avoiding the need for repeated x-rays to obtain adequate views. Employing simultaneous biplanar fluoroscopy for pinning of slipped capital femoral epiphysis, Westberry et al. showed improved precision in comparison to using a single C-arm.8 The authors have transitioned to the routine use of biplanar fluoroscopy for other knee procedures, including physeal bar excision, coronal or sagittal plane hemiepiphysiodesis with tension-band plates, or fracture fixation.
Summary
Anterior distal femoral hemiepiphysiodesis is a simple and effective technique to address knee flexion contractures common in neuromuscular conditions while minimizing surgical morbidity and patient discomfort. The use of a simultaneous dual C-arm technique facilitates operating room efficiency, requires minimal setup, allows for precise positioning of implants, all without compromising visualization or accuracy. We have reviewed the technique, its indications, pearls and pitfalls, and suggest this adjunct to improve intraoperative execution.
Acknowledgements
Thank you to Meaghan Hetherton Lyon for assistance with illustrations, © Copyright Andrew G. Georgiadis, MD.
Disclaimer
No funding was received. The authors have no conflicts of interest to disclose pertaining to this manuscript.
References
- Chang WN, Tsirikos AI, Miller F, et al. Distal hamstring lengthening in ambulatory children with cerebral palsy: primary versus revision procedures. Gait Posture. 2004;19(3):298–304.
- Klatt J, Stevens PM. Guided growth for fixed knee flexion deformity. J Pediatr Orthop. 2008;28(6):626-631.
- Kramer A, Stevens PM. Anterior femoral stapling. J Pediatr Orthop. 2001;21(6):804-807.
- Nazareth A, Gyorfi MJ, Rethlefsen SA, et al. Comparison of plate and screw constructs versus screws only for anterior distal femoral hemiepiphysiodesis in children. J Pediatr Orthop B. 2020;29(1):53-61.
- Kay RM, Rethlefsen SA. Anterior percutaneous hemiepiphysiodesis of the distal aspect of the femur: a new technique: a case report. JBJS Case Connect. 2015;5(4):e95.
- Long JT, Laron D, Garcia MC, et al. Screw anterior distal femoral hemiepiphysiodesis in children with cerebral palsy and knee flexion contractures: a retrospective case-control study. J Pediatr Orthop. 2020;40(9):e873-e879.
- Wang KK, Novacheck TF, Rozumalski A, et al. Anterior guided growth of the distal femur for knee flexion contracture: clinical, radiographic, and motion analysis results. J Pediatr Orthop. 2019;39(5):e360-e365.
- Westberry DE, Davids JR, Cross A, et al. Simultaneous biplanar fluoroscopy for the surgical treatment of slipped capital femoral epiphysis. J Pediatr Orthop. 2008;28(1):43-48.