
Original Research
Thoracolumbar Injury Classification and Severity Scale Can Help Identify Intra-Abdominal Injury in Children Injured in an MVC
1School of Medicine, Vanderbilt University, Nashville, TN; 2Duke University School of Medicine, Durham, NC; 3Department of Orthopaedics, Vanderbilt University Medical Center, Nashville, TN; 4Department of Surgery and Perioperative Care, Dell Medical School, University of Texas at Austin, Department of Orthopedic Surgery, Central Texas Pediatric Orthopedics, Austin, TX; 5Division of Pediatric Orthopaedics, Monroe Carell Jr. Children’s Hospital at Vanderbilt, Nashville, TN; 6Department of Pediatric Surgery, Vanderbilt University Medical Center, Nashville, TN; 7Department of Pharmacology, Vanderbilt University, Nashville, TN; 8Department of Pediatrics, Vanderbilt University Medical Center, Nashville, TN; 9Department of Pathology, Microbiology, and Immunology, Vanderbilt University Medical Center, Nashville, TN; 10Center for Bone Biology, Vanderbilt University Medical Center, Nashville, TN
Correspondence: Craig R. Louer Jr., MD, Department of Pediatric Orthopaedics, Monroe Carell Jr. Children’s Hospital at Vanderbilt, 2200 Children’s Way, Nashville, TN 37232. E-mail: [email protected]
Received: May 11, 2022; Accepted: October 13, 2022; Published: February 1, 2023
Volume 5, Number 1, February 2023
Abstract
Background: Motor vehicle crashes (MVC) cause variable injury to the thoracolumbar (TL) region of children secondary to rapid deceleration from seatbelts. This mechanism can also predispose a child to intraabdominal injury (IAI), which necessitates early diagnosis to limit morbidity and mortality. While the maximum extent of TL spine injury can be appreciated shortly after presentation, the severity of IAI may not be appreciated until days later. It is hypothesized that a measure of TL-injury severity will identify patients at risk of concomitant IAI.
Methods: Retrospective chart review identified 72 children with MVC-related TL spine injuries from 2007-2020. Patients were grouped based on the presence of IAI and TL spine injury (N=33) compared to isolated TL spine injury (no IAI, N=39). TL spine injury severity was classified according to the Thoracolumbar Injury Classification and Severity Scale (TLICS).
Results: Demographics were similar in both groups. Children with concomitant IAI had primarily lumbar spine injuries, while injuries without associated IAI were more broadly distributed throughout the thoracolumbar spine. Children without concomitant IAI were more likely to sustain compression fractures (n=31, 79%), while children with IAI had more distraction injuries (n=24, 73%). TL injuries associated with IAI were significantly more severe than isolated TL injuries (median TLICS=7 [range: 1-9] vs. 1 [range: 1-10], p<0.001). As hypothesized, increasing TLICS is associated with an increased risk of concomitant IAI, such that for every point increase in TLICS, the risk of IAI increases 49% (OR: 1.492, [95% CI 1.254-1.817], AROC 0.795).
Conclusions: Given the association between severe spine injury and IAI, this study examines the utility of TLICS score at presentation to establish an index of suspicion for concomitant IAI. While other clinical signs may be suggestive of the presence of IAI, our study may provide clinicians with another data point suggestive of spine injury severity in their diagnostic toolbox to optimally manage pediatric patients after MVC.
Level of Evidence: III, Retrospective Cohort Study
Key Concepts
- Pediatric patients are at risk for sustaining seatbelt syndrome (intraabdominal injury (IAI) associated with spinal column injury) after motor vehicle collisions when restraints are used improperly.
- Occult IAIs may not be readily diagnosed with initial trauma workup and require a high index of suspicion to avoid delay in diagnosis and potential morbidity and mortality.
- IAI is more frequently associated with spine fractures located in the lumbar spine.
- IAI is associated with more severe spine injury (represented by Thoracolumbar Injury Classification and Severity Scale [TLICS] score >5).
Introduction
Traumatic thoracolumbar (TL) spine injuries are rare in children, accounting for 2-5% of all spine trauma;1 however, they cause significant morbidity and mortality. Motor vehicle crashes (MVC) are the most common mechanism of pediatric TL spine trauma, causing 33-58% of injuries.1–3 MVCs cause variable injury to the TL region of children and present unique considerations for diagnosis and management. In addition to spinal injury, children are at high risk of experiencing intrabdominal injury (IAI) from MVCs.4–6 During rapid deceleration in an MVC, the abdominal organs are compressed between the seatbelt anteriorly and the bony vertebral column posteriorly.3 This mechanism can predispose a child to a well-known injury pattern, the seatbelt syndrome: a triad of spinal injury, IAI, and abdominal wall ecchymosis (AWE).4,7–10
In patients with blunt abdominal trauma caused by MVCs, solid organ injuries are commonly identified and diagnosed on cross-sectional imaging.12 Patients with hollow viscous injuries, however, may present with more subtle clinical findings, and injury is often not immediately evident on imaging, leading to delays in diagnosis of hollow viscous IAI.11–15 Though the presence of an AWE, also known as the seatbelt sign, is a predictor of underlying abdominal pathology, not all patients with IAI have a seatbelt sign,7–9 thereby making the identification of abdominal injury after MVC challenging.
At the time of presentation after MVC, hollow viscous IAI may not be clinically detectable and can evolve after admission, requiring regular evaluation, monitoring of clinical signs, and repeated imaging.11–16 Although the extent of IAI may not be obvious at initial presentation, the maximum extent of TL spine injury occurs at the time of MVC and is often diagnosed with initial workup. This study seeks to determine if the severity of the TL spine injury, as measured by the Thoracolumbar Injury Classification and Severity Scale (TLICS), is associated with concomitant IAI in pediatric patients after MVC, with the hypothesis that a more severe spinal injury increases the risk of concomitant IAI.
Materials and Methods
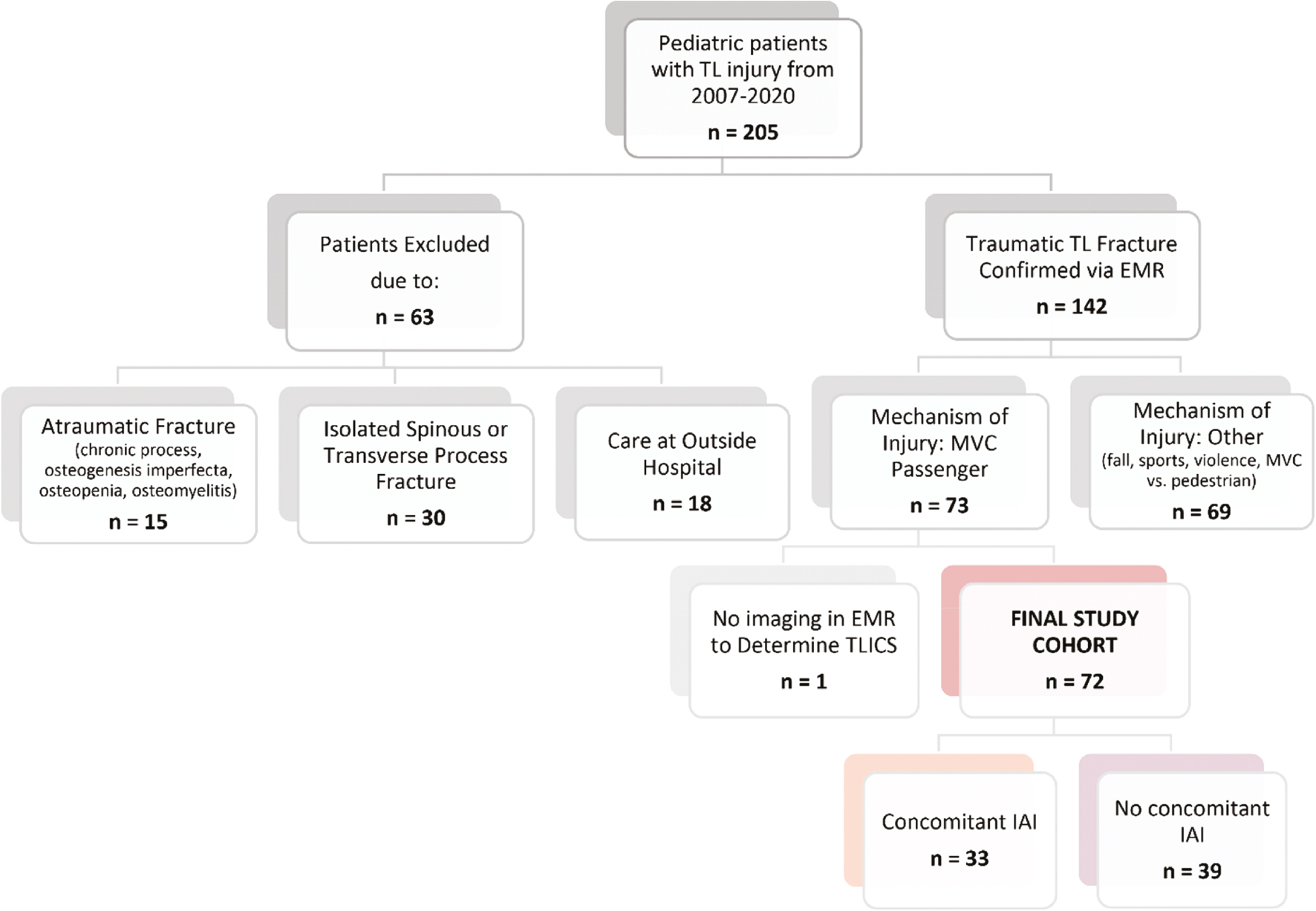
Following approval by the Institutional Review Board (IRB), a retrospective cohort study was conducted at a single, large, tertiary pediatric hospital. This study included patients younger than 18 years of age, presenting to the emergency department (ED) with traumatic TL spine injury after a motor vehicle crash (MVC) between January 2007 and June 2020. A total of 205 patients with TL spine injury were identified using our institution’s pediatric trauma registry (database spans 2016-2020) supplemented with data prior to 2016 with the following ICD-9 (805, 806) and CPT codes (22305, 22310, 22315, 22318, 22325-22327, 22842-22844). Presence of TL injury was confirmed via retrospective review of the electronic medical record (EMR). Of those, 63 were excluded due to atraumatic injury, isolated transverse or spinous process fractures, or primary management provided at an outside hospital; 69 patients were excluded due to mechanisms of injury other than MVC passenger (Figure 1). The patient population was divided into two subgroups based upon the presence or absence of concomitant IAI, defined as any injury involving the spleen, liver, pancreas, urinary tract, adrenal glands, or GI tract identified during the patient’s ED stay or hospitalization.
Figure 1. Patient consort diagram. TL = thoracolumbar, EMR = electronic medical record, MVC = motor vehicle crash, TLICS = Thoracolumbar Injury Classification and Severity Scale, IAI = intraabdominal injury.
The EMR of each patient was reviewed to determine patient demographics at the time of admission (age, sex, race, body mass index [BMI], Glasgow Coma Scale [GCS]), injury severity (initial imaging, level of spine injury, presence of IAI or abdominal wall ecchymosis, and neurologic status), and restraint status. Use of seatbelt restraint was determined using Emergency Medical Service (EMS) notes in the EMR; if no EMS note was available, patients were defined as unknown restraint status. Patients were restrained if EMS noted the use of any seatbelt: restrained, lap belt only, lap and shoulder belt, booster seat, or car seat. Patients were considered not restrained if lack of restraint was explicitly noted by EMS. Proper implementation of restraint device was unable to be verified. Treatment data for spine and abdominal injuries were collected. Postoperative complications, hospital and ICU lengths of stay, days in inpatient rehab, and hospital readmission data were also collected. Severity of TL spine injury was established using x-ray, CT, and MRI imaging based on the TLICS, a validated scale in both adults and pediatrics.16,17 All patients received at least one abdomen/pelvis CT scan as part of our institution’s standard trauma work-up. TLICS is a reliable and comprehensive system to describe TL spine trauma, stratify injury severity, and guide treatment. TLICS classifies the worst level of injury on a numerical scale of points based on fracture morphology (compression=1 point, translation/rotation=3 points, distraction=4 points), neurologic status (intact=1, nerve root injury=2, incomplete spinal cord=2, complete spinal cord=3, cauda equina=3), and integrity of the posterior ligamentous complex (intact=0, suspected/indeterminate=2, disrupted=3). Injuries are graded on a scale; scores ≤3 indicates nonsurgical management, a score of 4 suggests surgeon’s choice of management, and scores ≥5 indicate surgical management (Table 1).
Table 1. Thoracolumbar Injury Classification and Severity Scale16
| Injury Category | Point Value |
|---|---|
| Fracture Morphology | |
| Compression | 1 |
| Burst | 2 |
| Translation or rotation | 3 |
| Distraction | 4 |
| PLC Status | |
| Intact | 0 |
| Injury suspected or indeterminate | 2 |
| Injured | 3 |
| Neurologic Status | |
| Intact | 0 |
| Nerve root involvement | 2 |
| Spinal cord or conus medullaris injury | |
| Incomplete | 3 |
| Complete | 2 |
| Cauda equina syndrome | 3 |
| Outcomes | |
| Nonsurgical | 0-3 |
| Surgeon’s choice | 4 |
| Surgical | ≥5 |
The primary outcome of this study was the ability of TL injury severity, as defined by TLICS, to identify patients at risk for concomitant IAI. Patients were divided into two cohorts based on the presence or absence of IAI. Diagnosis of IAI was made via imaging or findings during explorative laparoscopy or other abdominal surgery. Continuous variables are presented as medians with standard deviations, and categorical variables are depicted as percentages. Statistical significance for continuous variables was calculated using non-parametric, Mann-Whitney, or Kruskal Wallis tests, given that data was found to be non-normally distributed. Categorical variables were analyzed with a chi-squared or Fisher’s exact test where appropriate. When evaluating TLICS’ or AWE ability to identify patients at risk of concomitant IAI, a simple logistic regression was used where IAI=1 and no-IAI=0 vs. TLICS values and/or AWE where 1=yes, and 0=no. Nagelkerke R2 and Wald statistic are reported. A likelihood ratio test was conducted on the three models to determine if univariate models (TLICS or AWE) or a combined model (TLICS+AWE) best predicted IAI in this patient population. A significance level of P<0.05 was applied for the entirety of the manuscript.
Results
Across the study period, 73 pediatric patients presented to the emergency department with TL spine injury after MVC. One patient was excluded from analysis because imaging was not available to determine TLICS grade, resulting in a total of 72 patients in the study population. Of these, 33 (46%) patients sustained concomitant IAI (Figure 1).
Patients with and without IAI were similar in age, race, ethnicity, gender, BMI, and GCS (Tables 2 and 3) yet differed in use of seatbelt restraint and varied markedly in their spinal injury patterns. Patients with IAI were more likely to be restrained than those without abdominal injury (88% and 72%, respectively, p=0.046). Frequency of injuries at each level of the thoracic and lumbar spine is shown in Figure 2. Children with concomitant IAIs experienced primarily lumbar injuries (L1-L5), while children without IAI experienced a spectrum of injuries throughout the thoracic and lumbar spine (Figure 2). There was no difference between children with and without IAI regarding rates of associated cervical spine injury (6% and 3%, respectively, p=0.590). Furthermore, when considering the level of worst injury in the TL spine (for which TLICS grade was assigned), children without IAI were more likely to sustain compression fractures (n=32, 82%), while patients with IAI were more likely to have distraction injuries (n=24, 73%) (p<0.001) (Table 3). Though both cohorts had high rates of lumbar spine injuries, when isolating lumbar injuries alone, the significant difference in fracture morphology persisted (p<0.001) (Table 4).
Table 2. Cohort Characteristics
| Total (n=72) | No IAI (n=39) | IAI (n=33) | p-value | |
|---|---|---|---|---|
| Gender, n (%) | 0.486 | |||
| Female | 34 (47.2%) | 20 (51.3%) | 14 (42.4%) | |
| Male | 38 (52.8%) | 19 (48.7%) | 19 (57.6%) | |
| Race, n (%) | 0.099 | |||
| White | 51 (70.8%) | 30 (76.9%) | 21 (63.6%) | |
| African American | 14 (19.4%) | 5 (12.8%) | 9 (27.3%) | |
| Asian | 4 (5.6%) | 1 (2.6%) | 3 (9.1%) | |
| Unknown | 3 (4.2%) | 3 (7.7%) | 0 (0%) | |
| Ethnicity, n (%) | 0.264 | |||
| Non-Hispanic | 63 (87.5%) | 33 (84.6%) | 30 (90.9%) | |
| Hispanic | 3 (4.2%) | 1 (2.6%) | 2 (6.1%) | |
| Unknown | 6 (8.3%) | 5 (12.8%) | 1 (3.0%) | |
| Age, yrs (median [range]) | 9.47 [1.56-17.71] | 10.46 [1.56-17.71] | 8.25 [3.28-17.29] | 0.223 |
| BMI (median [range]) | 18.70 [10.91-33.53] | 18.14 [10.91-33.53] | 19.52 [11.06-28.50] | 0.775 |
Table 3. Injury Severity
| Total (n=72) | No IAI (n=39) | IAI (n=33) | p-value | |
|---|---|---|---|---|
| TLICS: median (range) | 4 (1-10) | 1 (1-10) | 7 (1-9) | <0.001 |
| Fracture Morphology: n (%) | <0.001 | |||
| Compression fractures | 40 (55.6%) | 31 79.5% | 9 (27.3%) | |
| Flexion-Distraction fractures | 32 (44.4%) | 8 20.5% | 24 (72.7%) | |
| GCS (median [range]) | 15 [3-15] | 15 [5-15] | 15 [3-15] | 0.015 |
| Neurologic status: n (%) | 0.013 | |||
| Intact | 61 (84.7%) | 38 (97.4%) | 23 (69.7%) | |
| Transient | 0 (0%) | 0 (0%) | 0 (0%) | |
| Incomplete Cord | 2 (2.8%) | 0 (0%) | 2 (6.1%) | |
| Complete Cord | 8 (11.1%) | 1 (2.6%) | 7 (21.2%) | |
| Cannot Be Determined | 1 (1.4%) | 0 (0%) | 1 (3.0%) |
Figure 2. Distribution of thoracolumbar injuries in each cohort. All levels of injury are recorded here; thus, if a patient injured their spine at L1, L2, and L3, each level of injury is considered “involved” and represented in this figure.

Table 4. Lumbar Injuries in Each Cohort
| Total (n=49) | No IAI (n=22) | IAI (n=27) | p-value | |
|---|---|---|---|---|
| TLICS: median (range) | 6 (1-10) | 1 (1-10) | 7 (1-9) | <0.001 |
| Fracture Morphology: n (%) | <0.001 | |||
| Compression fractures | 24 (49.0%) | 17 (77.3%) | 7 (25.9%) | |
| Flexion-Distraction fractures | 25 (51.0%) | 5 (22.7%) | 20 (74.1%) |
Of the 39 patients without IAI, 38 were neurologically intact at presentation while one presented with complete spinal cord injury. Of the 33 patients with concomitant IAI, 23 were neurologically intact, two had incomplete spinal cord injuries, seven had complete spinal cord injuries, and one could not be determined due to diffuse axonal injury and brainstem injury (Table 3). Patients with IAI were more likely to have a neurologic injury and worse neurologic status at presentation (p=0.013). Neurologic status was consistent between presentation and discharge in all patients.
Among the 33 patients with concomitant IAI, eight patients (24%) did not have an abdominal wall ecchymosis (Table 5). Of the eight patients without AWE, median TLICS score was 7 (range 1-8); five patients had distraction spine injuries and three patients had compression fractures. The most common abdominal injury involved the small bowel (n=21, 64%), followed by the large bowel (n=16, 49%), and liver (n=7, 21%). The majority of patients underwent operative intervention for their abdominal injury (n=20, 61%) with 15 patients undergoing a laparotomy, four patients undergoing a laparoscopy converted to laparotomy, and one patient undergoing a laparoscopy.
Table 5. Intraabdominal Injury Characteristics
| Patients with Concomitant IAI (n=33) | |
|---|---|
| Injury type: n (%) | |
| Small Bowel | 21 (63.6%) |
| Colon | 16 (48.5%) |
| Liver | 7 (21.2%) |
| Spleen | 5 (15.2%) |
| Kidney(s) | 5 (15.2%) |
| Vasculature | 1 (3.0%) |
| Other | 10 (30.3%) |
| Abdominal wall ecchymosis: n (%) | |
| Yes | 25 (75.8%) |
| No | 8 (24.2%) |
| Operative intervention: n (%) | |
| None | 13 (39.4%) |
| Laparoscopy | 1 (3.0%) |
| Laparoscopy converted to laparotomy | 4 (12.1%) |
| Laparotomy | 15 (45.5%) |
| Multiple abdominal operations: n (%) | 2 (6.1%) |
Median TLICS grade for the entire population was 4 (range: 1-10). Patients with concomitant IAI had significantly more severe TL injuries as compared to patients with isolated TL spine injuries (median TLICS: 7 vs. 1, p<0.001) (Figure 3). Further, when isolating only the lumbar spine injuries, the difference in TLICS values persisted with IAI patients experiencing significantly more severe lumbar injuries (p<0.001) (Table 4). The TLICS scale designates scores ≥5 as severe injuries that likely necessitate spine surgery (Table 1). Using the value of ‘5’ as a demarcation point, most patients with IAI had TLICS values ≥5 (79%), while the majority of patients without IAI had TLICS values <5 (80%).
Figure 3. Severity of spine injury in each cohort. TLICS grade was assigned at the level of worst injury; thus, each patient received only one TLICS grade regardless of how many levels of the spine were injured. ****, P<0.001.

A higher TLICS score upon admission was positively associated with an increased risk of concomitant IAI, such that for every point increase in TLICS, the risk of IAI increased 49% (OR: 1.492, [95% CI 1.254-1.817], AROC 0.795, Nagelkerke R2=0.384). Likewise, the occurrence of AWE was positively associated with an increased risk for concomitant IAI (OR: 1.719, [95% CI 0.7225-2.798], AROC 0.699, Nagelkerke R2=0.203). Comparing these two variables, TLICS was a stronger predictor of IAI with a Wald statistic of 15.79 compared to 6.32 for AWE. When included together the model of TLICS and AWE outperformed either individual model (AROC 0.861, Nagelkerke R2=0.469), which was confirmed by conducting a likelihood ratio test (TLICS vs. TLICS+AWE, deviance=6.734, p=0.009; AWE vs. AWE+TLICS, deviance=19.273, p<0.001.)
Aligning with more severe spine injuries as noted by TLICS, patients with IAI were significantly more likely than those without IAI to undergo operative fixation of their spinal fracture (n=22 vs. 5, p<0.001), spend more time in the hospital (11 vs. 2 days, p<0.001), spend more time in the ICU (3 vs. 0 days, p<0.001), and spend more time in inpatient rehab (p=0.003). There was no significant difference between the cohorts regarding readmission rates (Table 6).
Table 6. Clinical Outcomes
| Total (n=72) | No IAI (n=39) | IAI (n=33) | p-value | |
|---|---|---|---|---|
| Spinal Injury Management: n (%) | <0.001 | |||
| Non-operative | 45 (62.5%) | 34 (87.2%) | 11 (33.3%) | |
| Operative | 27 (37.5%) | 5 (12.8%) | 22 (66.7%) | |
| Hospital Days (median [range]) | 5 | 2 [1-10] | 11 [2-104] | <0.001 |
| ICU Days (median [range]) | 0 [0-34] | 0 [0-9] | 3 [0-34] | <0.001 |
| Days in Inpatient Rehab (median [range]) | 0 [0-210] | 0 [0-38] | 0 [0-210] | 0.003 |
| Hospital Readmission, n (%) | 3 (3.9%) | 0 (0%) | 3 (9.1%) | 0.088 |
Discussion
This study examined the largest singular cohort of pediatric patients with spine injury after an MVC and is the first study to explore the relationship between TL spine injury severity, as measured by TLICS, and incidence of IAI. In this cohort, 46% of patients sustained both TL spine injuries and IAIs. Patients with concomitant IAI tended to have predominantly lumbar spine injuries, flexion-distraction fractures, worse neurologic status, and more severe spine injuries as graded by TLICS. Previously, TLICS has been validated in the pediatric population to determine fracture stability and guide surgical decision-making.1,2,16,17 Results from this study align with prior validation studies demonstrating that patients with higher TLICS grades are more likely to need operative fixation of their spine and spend longer in the hospital and ICU. This study adds new data to the body of prior literature by being the first study to demonstrate that the severity of spine injury increases in patients with concomitant IAI and that a higher TLICS score upon admission, particularly a score ≥5, is associated with an increased risk of IAI.
While seatbelts are protective in car accidents against fatality and overall injury severity, their use is associated with a well-defined injury pattern. Beginning in the 1960s, the term seatbelt syndrome was coined to describe the spectrum of injuries that occur due to lap belts in MVCs: TL spine injury, IAI, and AWE.18 As the forward velocity of the car stops abruptly in an MVC, the occupant continues to move forward and folds over the seatbelt, which acts as a fulcrum.3 Children are particularly susceptible to this pattern of injury as their seatbelts tend to ride up over the mid-abdomen and they have an increased force of flexion across the belt due to a higher center of gravity caused by an increased head-to-body ratio.2,3,5,6 This study corroborates the mechanism causing seatbelt syndrome as patients with IAI and TL spine injury were more likely to be restrained by seatbelt than those patients without IAI. Aligning with this mechanism of injury, this study and prior published studies have reported that patients with concomitant IAI have predominantly lumbar, flexion-distraction injuries.2,7,10,19,20 Likewise, IAI and AWE occur from compression between the belt anteriorly and the spinal column posteriorly, shear across the fixed seatbelt, or from rapid increases in intraluminal pressure that can rupture bowel walls.20 Given this mechanistic association, AWE is one of the hallmark indications of patients at high risk of IAI, as shown in this study and in priors.8,21–23 However, to the authors’ knowledge, this study is the first and only to show that TLICS is a stronger predictor of IAI than AWE. Furthermore, not all patients with IAI have AWE6,8,10,23 and some studies report no increased risk of IAI in patients with AWE.24,25 In this study, 22% of patients with IAI had no AWE noted in their chart. TLICS can be a valuable tool in patients without AWE to indicate risk of concomitant IAI; however, even in patients with AWEs, this study demonstrates that combining TLICS and AWE is a stronger predictor of concomitant IAI than AWE alone.
Identifying IAI in a child following an MVC can be challenging. While a physical exam may reveal concerning signs, children with IAI caused by blunt trauma, especially hollow viscous injuries, may have subtle, equivocal, or absent physical exam findings.6,8,23–25 Furthermore, if the patient has significant associated traumatic head injury and neurologic compromise, clinical examination and feedback may be limited. FAST (Focused Assessment with Sonography in Trauma) exams have shown to have mixed utility in identifying solid organ injury, are unable to identify hollow viscous injuries, and are not consistently used in the pediatric population.26 Even on CT scan, hollow viscous injuries can be subtle and nonspecific;6,10,19 the sensitivity of CT to traumatic bowel injury varies from 69-92%.27 Given the limitations of physical exam and imaging to diagnose traumatic IAI, this study demonstrated how providers can use imaging and assessment of the spine trauma at the time of presentation to help establish a high index of suspicion for concomitant IAI and a low threshold for further diagnostic evaluation and management of such patients. While the sole presence of lumbar fractures should increase suspicion of IAI after MVC,10,19,28–30 not all patients with lumbar fractures have an IAI. Importantly, this study is the first to show the strong association between the severity of TL fractures, as indicated by the TLICS score, and the presence of IAI. For each point increase in a patient’s TLICS score, their risk of IAI increases by 49%.
Prior published case reports and retrospective studies have noted the challenges in identifying intra-abdominal injuries due to seatbelts and highlighted examples in which intra-abdominal injuries in seatbelt syndrome patients were missed on initial presentation.13–15 Though this study did not identify any additional IAI as a result of TL spine injury severity, this select cohort was not powered to detect rare events such as delayed diagnosis. Given the noted challenges in diagnosing traumatic IAI, TLICS represents an additional, valuable, data point in a treating physicians’ armamentarium to help optimally manage pediatric patients after MVC.
Study Strengths & Limitations
This study has several strengths and limitations. While the retrospective nature of this study allows us to evaluate a larger cohort than many prior studies, this study was limited to the data collection that was available in the EMR. In particular, data on the use of seatbelt restraints in this population was dependent on notation in the EMR by emergency medical services (EMS). While EMS noted restraint vs. no restraint in 93% of patients, they did not reliably include data indicating the appropriateness of use, nor the distinction of car seats or booster seats. While documentation of proper seatbelt use was not captured, the presence of seatbelt signs in 78% of patients with IAI indicates usage of seatbelts. TLICS as a clinical tool does not rely on the proper use of a seatbelt and often the clinical providers are unaware of restraint status in these patients; thus, evaluation of the spine is standardized regardless of seatbelt usage. Additionally, this study was focused on patients with spine injury after MVC and did not collect data on MVC patients with IAI but no spine injury. Future, prospective studies would be needed to explore the true predictive value of TLICS in patients with IAI, independent of the mechanism of injury. Finally, this is a retrospective study conducted at a single institution which may limit generalization; however, this relatively large cohort of pediatric patients with spine injury after MVC supports data reported by other studies.7,8,18,19
Conclusions
Success in the management of pediatric trauma following MVC is dependent on awareness of injury patterns as well as the availability of clinical tools to assist in the diagnosis and management of this spectrum of injuries. Given our findings of the association between TL spine injury and IAI, this study demonstrates how TLICS can be an additional, valuable, clinical tool to establish a high index of suspicion for concomitant IAI when managing pediatric patients with spine trauma following MVC. TLICS score outperformed prior hallmark indicators of identifying IAI, such as AWE. For patients without AWE or equivocal imaging and physical exam or in clinical scenarios where CT scans are less common, a higher TLICS can identify those requiring additional scrutiny, such as repeated abdominal workup, imaging, or longer length of stay for observation. Our study provides clinicians with a new data point, specifically spine injury as graded by TLICS, to help manage pediatric patients after MVC.
Acknowledgement
The authors would like to thank members of the Division of Pediatric Orthopaedics for their care of patients at our institution; this work would not have been possible without their dedication. Additionally, we would like to thank our family and friends for their continued support and understanding.
Disclaimer
Funding for this study was supported by the Caitlin Lovejoy Fund, the Vanderbilt University Medical Center Department of Orthopaedics, and the Vanderbilt School of Medicine Research Immersion program. Creation of the retrospective database utilized in this study was supported by CTSA award No. UL1 TR002243 from the National Center for Advancing Translational Sciences. The authors report no conflicts of interest related to this manuscript.
References
- Daniels AH, Sobel AD, Eberson CP. Pediatric thoracolumbar spine trauma. J Am Acad Orthop Surg. 2013;21(12):707-716.
- Srinivasan V, Jea A. Pediatric thoracolumbar spine trauma. Neurosurg Clin N Am. 2017;28(1):103-114.
- Achildi OE, Betz R, Grewal H. Lapbelt injuries and the seatbelt syndrome in pediatric spinal cord injury. J Spinal Cord Med. 2007;30(suppl 1):S21-S24.
- Newman KD, Bowman LM, Eichelberger MR, et al. The lap belt complex: intestinal and lumbar spine injury in children. J Trauma. 1990;30(9):1133-1140.
- Agran P, Winn D, Dunkle D. Injuries among 4- to 9-year-old restrained motor vehicle occupants by seat location and crash impact site. Am J Dis Child. 1989;143(11):1317-1321.
- Santschi M, Echavé V, Laflamme S, et al. Seat-belt injuries in children involved in motor vehicle crashes. Can J Surg. 2005;48(5):373-376.
- Beaunoyer M, St-Vil D, Lallier M, et al. Abdominal injuries associated with thoraco-lumbar fractures after motor vehicle collision. J Pediatr Surg. 2001;36(5):760-762.
- Borgialli DA, Ellison AM, Ehrlich P, et al. Association between the seat belt sign and intra-abdominal injuries in children with blunt torso trauma in motor vehicle collisions. Acad Emerg Med. 2014;21(11):1240-1248.
- Vailas MG, Moris D, Orfanos S, et al. Seatbelt sign in a case of blunt abdominal trauma; what lies beneath it? BMC Surg. 2015;15(1):121.
- Sivit CJ, Taylor GA, Newman KD, et al. Safety-belt injuries in children with lap-belt ecchymosis: CT findings in 61 patients. AJR Am J Roentgenol. 1991;157(1):111-114.
- Bala M, Adileh M, Almogy G, et al. Abdominal injury patterns in patients with seatbelt signs requiring laparotomy. J Emerg Trauma Shock. 2014;7(4):295-300.
- Mackersie RC, Tiwary AD, Shackford SR, et al. Intra-abdominal injury following blunt trauma: identifying the high-risk patient using objective risk factors. Arch Surg. 1989;124(7):809-813.
- Taylor GM, Zygowiec JP, Wallace LC, et al. Perforated small intestine: a case of a delayed presentation of an intra-abdominal injury in a pediatric patient with a seatbelt sign. Clin Med Insights Pediatr. 2019;13:117955651987663.
- Al-Ozaibi L, Adnan J, Hassan B, et al. Seat belt syndrome: delayed or missed intestinal injuries, a case report and review of literature. Int J Surg Case Rep. 2016;20:74-76.
- Dodds M, Gul R, Cassidy N. Late-diagnosed seat-belt syndrome: a second chance? Inj. Extra. 2006;37:25-27.
- Bono CM, Vaccaro AR, Hurlbert RJ, et al. Validating a newly proposed classification system for thoracolumbar spine trauma: looking to the future of the thoracolumbar Injury classification and severity score. J Orthop Trauma. 2006;20(8):567-572.
- Dawkins RL, Miller JH, Menacho ST, et al. Thoracolumbar injury classification and severity score in children: a validity study. Neurosurgery. 2019;84(6):E362-E367.
- Garrett JW, Braunstein PW. The seat belt syndrome. J Trauma. 1962;2(3):220-238.
- Mulpuri K, Reilly C, Perdios A, et al. The spectrum of abdominal injuries associated with chance fractures in pediatric patients. Eur J Pediatr Surg. 2007;17(5):322-327.
- Le TV, Baaj AA, Deukmedjian A, et al. Chance fractures in the pediatric population: a review. J Neurosurg Pediatr. 2011;8(2):189-197.
- Anderson PA, Henley MB, Rivara FP, et al. Flexion distraction and chance injuries to the thoracolumbar spine. J Orthop Trauma. 1991;5(2):153-160.
- Sokolove PE, Kuppermann N, Holmes JF. Association between the “seat belt sign” and intra-abdominal injury in children with blunt torso trauma. Acad Emerg Med. 2005;12(9):808-813.
- Szadkowski MA, Bolte RG. Seatbelt syndrome in children. Pediatr Emerg Care. 2017;33(2):120-125.
- Chidester S, Rana A, Lowell W, et al. Is the “seat belt sign” associated with serious abdominal injuries in pediatric trauma? J Trauma. 2009;67(1 Suppl):S34-S36.
- Makrin V, Wiesel O, Heller D, et al. Low probability of significant intra-abdominal injury in stable patients with abdominal “seat belt sign”. Eur J Trauma Emerg Surg. 2009;35(4):403-406.
- Liang T, Roseman E, Gao M, et al. The utility of the focused assessment with sonography in trauma examination in pediatric blunt abdominal trauma: a systematic review and meta-analysis. Pediatr Emerg Care. 2021;37(2):108-118.
- Hassan R, Abd Aziz A. Computed tomography (CT) imaging of injuries from blunt abdominal trauma: a pictorial essay. Malays J Med Sci. 2010;17(2):29-39.
- Paris C, Brindamour M, Ouimet A, et al. Predictive indicators for bowel injury in pediatric patients who present with a positive seat belt sign after motor vehicle collision. Pediatr Surg. 2010;45(5):921-924.
- Anderson PA, Rivara FP, Maier RV, et al. The epidemiology of seatbelt-associated injuries. J Trauma. 1991;31(1):60-67.
- Rao RD, Berry CA, Yoganandan N, et al. Occupant and crash characteristics in thoracic and lumbar spine injuries resulting from motor vehicle collisions. Spine J. 2014;14(10):2355-2365.