
Surgical/Technical Tips
A Novel Technique to Remove Plaster Ponseti Clubfoot Casts
International Center for Limb Lengthening, Rubin Institute for Advanced Orthopedics, Sinai Hospital of Baltimore, Baltimore, MD
Correspondence: John E. Herzenberg, MD, International Center for Limb Lengthening, Rubin Institute for Advanced Orthopedics, Sinai Hospital of Baltimore, 2401 W. Belvedere Ave., Baltimore, MD 21215. E-mail: [email protected]
Received: June 13, 2022; Accepted: June 23, 2022; Published: August 1, 2022
DOI: 10.55275/JPOSNA-2022-0075
Volume 4, Number 3, August 2022
Abstract:
Serial Ponseti-style plaster of Paris casts are considered the gold standard treatment for clubfoot in infants. In conjunction with cast application, weekly cast removals are a necessary part of treatment, predisposing this patient population to cast saw injuries. Extensive research and education have been devoted to eliminating iatrogenic cast saw injuries. However, decreasing experience and familiarity with cast saws lead to a 1–2% incidence rate of cast saw burns or abrasions. While alternatives such as soaking the cast off or using protective strips are available, these lead to interruptions in clinic workflow and failure to successfully treat clubfoot, respectively. We present a technique that successfully and safely removes Ponseti-style plaster of Paris casts by perforating only the convex side of the cast, using superficial partial-thickness scores and a large cast spreader. The proposed technique can reduce cast saw injuries by potentially 50%.
Key Concepts:
- Cast saw injuries can involve abrasive and/or thermal injuries.
- Cast saw injuries are difficult to prevent due to the inherent risks of a cast saw.
- Infants undergoing clubfoot treatment with Ponseti-style casts are predisposed to cast saw injuries.
- We present a novel technique which reduces cast saw use in half by only perforating one side of the cast (univalve rather than the standard bivalve), therefore reducing risk of injury by 50%.
Introduction
The first accounts of clubfoot treatment by Hippocrates describe gentle serial manipulations and bandaging (circa 400 B.C.E.).1 Various stretching methods, forcible manipulations, and use of assorted mechanical devices were subsequently introduced.1 Early surgical procedures were limited to percutaneous tenotomies. The introduction of aseptic surgical techniques, anesthesia, and the pneumatic tourniquet at the end of the 19th century allowed the development of more radical operations that consisted of aggressive soft tissue releases and osteotomies.2 Unfortunately, such procedures were found to result in stiff, painful feet and high relapse rates.2 These poor results inspired Ponseti’s careful study of clubfoot pathophysiology and anatomy and in turn led to the development of his protocol of gentle serial manipulations and casting of clubfeet with plaster of Paris.
Plaster of Paris was initially introduced in 1798 by Napoleon’s surgeons as a method to immobilize wartime fractures. Plaster (and eventually fiberglass) casting have been an integral part of the orthopaedic surgeon’s armamentarium since their inception.3 Casting and cast removal have become less common due to the advent of safe and effective internal fixation of fractures, making them somewhat of a lost art.4 It is not uncommon for residents who utilize cast saws to begin doing so with less than 1 hour of formal training.5
The lack of routine familiarity with the methods can create a scenario for infants to suffer skin injuries (abrasions, cuts, and burns) during cast removal. During removal with a cast saw, patients are at risk of for these injuries. Cast saw burn rates ranges from 1.3 to 7.2 burns per 1,000 casts removed.6,7 The incidence of cast saw injuries has been recorded as high as 1.23% at a single institution.8 The oscillating cast saw, developed by Homer Stryker, is designed to cut hard material but not flexible surfaces that move with the saw, such as skin. The design has not changed much in nearly 80 years.
However, when applying pressure or dragging the saw, the skin becomes immobile and therefore at risk for abrasive injury. This may also occur around bony prominences such as the malleoli in which there is minimal subcutaneous fat.9 When cutting plaster, cast saws reach an average temperature of 52 degrees Celsius.10 Dull cast saw blades can reach temperatures of up to 66 degrees Celsius, temperatures at which a third-degree burn can occur in under 1 second.11 Children and the elderly are particularly sensitive to thermal injuries.12
A wide array of research and effort has been dedicated to preventing iatrogenic cast-removal injuries. Some institutions have proposed a zero-event policy.13 Several methods have been shown to reduce the incidence of cast saw injuries, including using appropriately sharp cast saw blades,6 intermittently inspecting the blade’s temperature and cooling it with water or alcohol,14 running the cast saw with a vacuum to clean debris and keep it cool,15 and positioning safety strips under the cast.16 Improving education around proper cast saw usage technique and the use of laboratory simulation has also been advocated as a means to reduce iatrogenic injuries.17,18 Despite education and increased experience, on average, practitioners made contact with a simulated patient’s skin 25 times, with one of those contacts on average lasting longer than 1 second, therefore posing a significant risk for thermal injury.13
We aim to reduce the risk of iatrogenic cast removal injuries with the presentation of a novel technique for removing long leg Ponseti clubfoot plaster casts. This method utilizes a univalve cut instead of a bivalve cut, which theoretically should cut the risk of injuries by 50% and uses both a small and large cast spreader. This technique may be used with any plaster cast.
Description of the Method
The following describes a modified technique for removal of a Ponseti-style clubfoot long leg plaster cast as demonstrated in the accompanying video. The child is positioned supine. Identify the convex side of the cast for the univalve. This will be the external side of the cast for the initial casts and the internal side for the later casts once the foot has crossed the midline and is externally rotated (Figure 1).
Figure 1. Four views of a child with his first set of bilateral plaster casts for idiopathic clubfoot. The solid lines on the convex side show where the full cut is made down to cotton padding. The dotted lines on the convex side show where the cast is scored. The transverse dotted lines anteriorly at the knee and posteriorly at the ankle represent scores of the plaster. (Copyright 2022, Rubin Institute for Advanced Orthopedics, Sinai Hospital of Baltimore. Used with permission.)

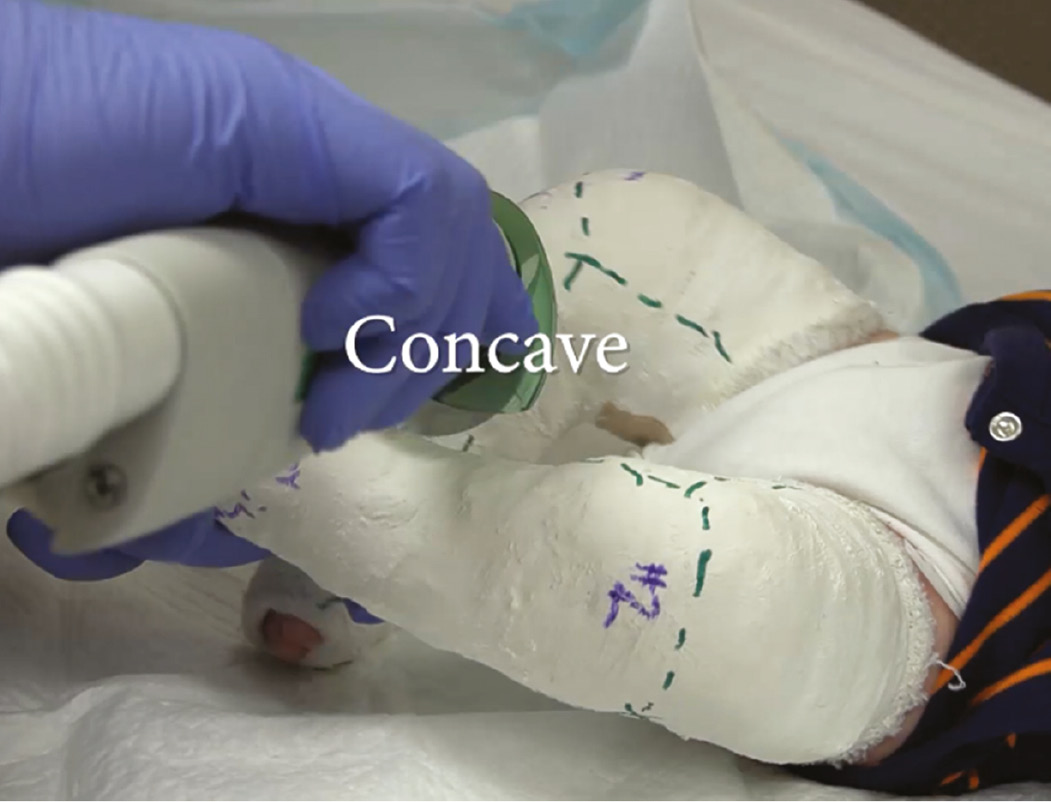
The concave side is deeper, less accessible, and therefore more prone to injury (Figure 2).6 The convex side is more accessible to the cast saw. By fully cutting the plaster down to cotton on the convex side of the cast with our technique, the concave portion of the cast, which is at higher risk of injury, is avoided.6 The child should be turned during the procedure so the cast portion being cut is facing upward. Studies have shown that with the patient in the lateral decubitus position, the lateral portion of the cast sits 16.2 mm above the skin on average as opposed to 13.7 mm if the patient is positioned supine.19,20
Figure 2. Demonstrating the difficulty of cutting the cast on the deep concave side. In our technique, this side is only scored, not fully cut. (Copyright 2022, Rubin Institute for Advanced Orthopedics, Sinai Hospital of Baltimore. Used with permission.)
Make three overlapping straight cuts (thigh, calf, foot) through the convex side, down to the cast padding. Next, make three overlapping straight shallow scores (2-3 mm deep) on the thigh, calf, and foot of the concave side, making no attempt to reach the cast padding. Next, make a shallow score anteriorly, across the knee, connecting the medial and lateral cuts. Finally, make a shallow score posteriorly, behind the ankle at the level of the Achilles tendon, connecting the medial and lateral cuts. In total, one full length full thickness cut, one full length score, and two transverse scores will have been made. The scores should be safe when made this shallow. The full thickness cut, being on only one side (univalve), should be safer than the usual full thickness bivalve cuts.
Whenever using the cast saw, always take the typical precautions. For the full thickness cuts, the cast is perforated using a proper “in-out” technique while stabilizing the cast saw with the index finger to allow precise control of the depth and pressure of the cast saw blade.5 The cast saw blade temperature is intermittently checked by holding it between two fingers. If the blade cannot be comfortably held for 5 seconds, sawing is paused until the blade is cooled (with water) to an appropriate temperature. The cast saw blade is advanced 1 to 2 cm after each penetration, ensuring the blade is completely removed between each penetration to allow clearance of debris and prevent the blade from dragging across the skin.
Once the convex side of the cast is completely perforated, a standard fine tooth cast spreader is inserted, and the cast is split gently along its convex, univalved side. Next, the medium or large cast spreader (Figure 3) is introduced to gently spread the cast width.
Figure 3. The initial spread of the univalve cut is made with the fine cast spreader. Use the large spreader, fully deployed, to complete the opening of the cast. (Copyright 2022, Rubin Institute for Advanced Orthopedics, Sinai Hospital of Baltimore. Used with permission.)

The additional anterior (knee) and posterior (ankle) scores make the cast easier to remove by encouraging it to crack open at those two levels. The large size cast spreader exerts enough leverage to crack the cast wide open (Figure 4).
Figure 4. The fully cut cast, spread wide, ready to extract the leg. (Copyright 2022, Rubin Institute for Advanced Orthopedics, Sinai Hospital of Baltimore. Used with permission.)

Most practitioners lack the significant finger strength required to split the univalve cast open without the large cast spreader. Both the fine tooth cast spreader and the medium cast spreader are readily available for purchase together, online from various vendors for approximately $40 USD (Figures 5A and 5B).
Figure 5. A) The small, medium and large cast spreaders. B) The small and medium cast spreaders, opened. The small spreader opens 18 mm, the medium opens 48 mm. C) The small versus large cast spreader, fully opened: 18 mm vs. 145 mm. (Copyright 2022, Rubin Institute for Advanced Orthopedics, Sinai Hospital of Baltimore. Used with permission.)

The less commonly available large cast spreader is available online and can be for purchased for approximately $50 USD (Figure 5C).
As usual, care is taken during the removal of any stockinette (if used) and cast padding (we recommend Webril; Cardinal Health, Dublin, OH) to avoid skin cuts with bandage scissors. See available video of the technique: http://www.kaltura.com/tiny/00dbf.
Comparison to Other Methods
Alternatives to cast saw use have been offered by others as means to prevent iatrogenic cast saw injuries. Some advocate soaking the cast in lukewarm water to remove the night before the clinic visit.21 While this does represent a safe approach, the risk of clubfoot relapse overnight without a cast is a concern when following the Ponseti method. It is preferable to remove the cast just before reapplying the new cast.22 Furthermore, soaking a cast off while in the office can lead to disruptions in clinic flow and delays.21 In several clinics, the cast is partially soaked, and then a very sharp linoleum knife is used to cut the partially softened gauze. This knife is both sharp and frightening. Others have suggested splitting plaster casts with a scalpel blade before it dries to allow for safer removal with a cast spreader and scissors.23 While in theory a scalpel should not cut the padding, this approach has only been tested on balloon models and no data is available on the incidence of scalpel injuries associated with this technique. Furthermore, some have suggested using foam padding as a means to limit cast saw injuries by increasing the distance between the cast and skin;24,25 however, bulky foam padding would not be amenable when using a cast to accurately hold a manipulated clubfoot. A commercially available cast saw safety strip is available but also adds bulk and expense. Plastic cutting protectors inserted into the cast between the skin and padding are not practical in small clubfoot baby casts. Finally, it should be mentioned that some Ponseti practitioners avoid plaster altogether in favor of semi-rigid synthetic fiberglass casting tape, although the moldability characteristics were not quite as good as plaster in a randomized clinical trial.26 Other researchers have found no difference between the efficacy of both materials and a parent preference towards semi-rigid fiberglass.27
Summary
Ponseti casting, the gold standard treatment of congenital clubfeet, requires weekly cast application and removal in a patient population that is at particular risk for thermal injuries due in part to the thin layer of padding advocated by Ponseti. Iatrogenic cast saw injuries can lead to significant injuries to our patients and a loss of trust of the patient and their families. There is no faster way to lose the confidence of a family than by injuring their child with a cast saw. They’re also associated with litigation fees which average $15,898 per patient.6,9,28 Therefore, increased awareness, training, and innovation are required to further reduce their incidence. The technique proposed theoretically reduces the cast saw’s use in half by only perforating one side of the cast (univalve rather than the standard bivalve), therefore also reducing risk of injury by 50%. Scoring the cast instead of making a second “valve” encourages the cast to crack open when the large spreader is applied.
By optimizing the technique of plaster cast removal, we aspire to reduce the incidence of iatrogenic injury. We have used this technique for several months in a busy weekly clubfoot clinic and have not observed any cast saw injuries. Verification of efficacy remains to be proven in prospective trials. This technique has only been used with plaster casts, not with standard fiberglass casts.
Additional Links
- POSNAcademy: Reducing Cast-Saw Injuries in Children: Novel Technique to Remove Plaster Ponseti Clubfoot Casts, Rubén Monárrez, MD; John E. Herzenberg, MD; Philip K. McClure, MD—http://www.kaltura.com/tiny/00dbf
- Cast Saw Burn Prevention: An Evidence-Based Review—https://pubmed.ncbi.nlm.nih.gov/33475304/6
Disclaimer
J. Herzenberg: Clinical advisor for Bonus BioGroup and a consultant for NuVasive Specialized Orthopedics, Orthofix, OrthoPediatrics, OrthoSpin, Smith & Nephew, and WishBone Medical. P. McClure: Consultant for DePuy Synthes Companies, Novadip, NuVasive Specialized Orthopedics, Orthofix, and Smith & Nephew. The following organizations supported the authors’ institution: DePuy Synthes, Integra LifeSciences, NuVasive Specialized Orthopedics, Orthofix, OrthoPediatrics, Paragon 28, Pega Medical, Smith & Nephew, Stryker, Treace Medical Concepts, and WishBone Medical Inc.
References
- Sanzarello I, Nanni M, Faldini C. The clubfoot over the centuries. J Pediatr Orthop B. 2017;26(2):143–151.
- Dobbs MB, Morcuende JA, Gurnett CA, et al. Treatment of idiopathic clubfoot: an historical review. Iowa Orthop J. 2000;20:59–64.
- DeMaio M, McHale K, Lenhart M, et al. Plaster: our orthopaedic heritage: AAOS exhibit selection. J Bone Joint Surg Am. 2012;94(20):e152.
- Maag ALD, Laufer S, Kwan C, et al. Sensor-based assessment of cast placement and removal. In: Studies in Health Technology and Informatics. Vol 196. IOS Press; 2014:259-261.
- Shuler FD, Grisafi FN. Cast-saw burns: Evaluation of skin, cast, and blade temperatures generated during cast removal. J Bone Joint Surg Am. 2008;90(12):2626-2630.
- Larson JE, Nicolay RW. Cast saw burn prevention: an evidence-based review. J Am Acad Orthop Surg. 2021;29(9):380-385.
- Ridley TJ, McCarthy MA, Bollier MJ, et al. The incidence and clinical outcomes of peroneal nerve injuries associated with posterolateral corner injuries of the knee. Knee Surg Sports Traumatol Arthrosc. 2018;26(3):806-811.
- Shore BJ, Hutchinson S, Harris M, et al. Epidemiology and prevention of cast saw injuries: results of a quality improvement program at a single institution. J Bone Joint Surg Am. 2014;96(4):e31.
- Halanski MA. How to avoid cast saw complications. J Pediatr Orthop. 2016;36(4):S1-S5.
- Steiner SRH, Gendi K, Halanski MA, et al. Efficiency and safety: the best time to valve a plaster cast. J Bone Joint Surg Am. 2018;100(8):e49.
- Killian JT, White S, Lenning L. Cast-saw burns: comparison of technique versus material versus saws. J Pediatr Orthop. 1999;19(5):683-687. Available at: https://journals-lww-com.proxy1.library.jhu.edu/pedorthopaedics/Fulltext/1999/09000/Cast_Saw_Burns__Comparison_of_Technique_Versus.26.aspx. Accessed April 20, 2022.
- Burghardt RD, Anderson JG, Reed RA, et al. Exothermic properties of plaster-synthetic composite casts. J Child Orthop. 2014;8(2):193-201.
- Monroe KC, Sund SA, Nemeth BA, et al. Cast-saw injuries: Assessing blade-to-skin contact during cast removal: does experience or education matter? Phys Sportsmed. 2014;42(1):36-42.
- Puddy AC, Sunkin JA, Aden JK, et al. Cast saw burns: evaluation of simple techniques for reducing the risk of thermal injury. J Pediatr Orthop. 2014;34(8):e63-e66.
- McNeil DS, Trenholm JAI. Establishing safety parameters for orthopaedic cast saw blade usage. J Pediatr Orthop. 2021;41(10):e884-e888.
- Stork NC, Lenhart RL, Nemeth BA, et al. To Cast, to Saw, and not to injure: can safety strips decrease cast saw injuries? Clin Orthop Relat Res. 2016;474(7):1543-1552.
- Ruder JA, Brighton BK, Vander Have KL, et al. Effectiveness of a low fidelity cast removal module in orthopaedic surgical simulation. J Surg Educ. 2018;75(5):1329-1332.
- Cameron J, Twedt M, Garvey J, et al. Novel cast-saw alarm system reduces blade-to-skin contact in a pediatric upper extremity model. J Pediatr Orthop. 2022;42(5):289-292.
- Abu-Ghanem Y, Steinberg EL, Maman E, et al. The anterior aspect is the safest area to split a leg cast in the supine position: a study protocol. Orthop Nurs. 2013;32(6):316-319.
- Abu-Ghanem Y, Abu-Ghanem N, Albagly A, et al. Limb position significantly affects safety distance during cast removal. Orthop Nurs. 2015;34(2):110-112.
- Sodhai VM, Patwardhan SA, Shyam AK, et al. Ponseti cast removal: video technique. J Orthop Case Rep. 2020;10(3):50-52.
- Terrazas-Lafargue G, Morcuende JA. Effect of cast removal timing in the correction of idipoathic clubfoot by the ponseti method. Iowa Orthop J. 2007;27:24-27.
- Sabat D, Kumar V. Splitting plaster with a scalpel blade: a safe way to allow easy splitting of a plaster [Injury 2008;39(3):368-70]. Injury. 2009;40(6):674.
- Seehausen DA, Kay RM, Ryan DD, et al. Foam padding in casts accommodates soft tissue swelling and provides circumferential strength after fixation of supracondylar humerus fractures. J Pediatr Orthop. 2015;35(1):24-27.
- Murgai RR, Compton E, Patel AR, et al. Foam padding in postoperative lower extremity casting: an inexpensive way to protect patients. J Pediatr Orthop. 2018;38(8):e470-e474.
- Pittner DE, Klingele KE, Beebe AC. Treatment of clubfoot with the Ponseti method: a comparison of casting materials. J Pediatr Orthop. 2008;28(2):250-253.
- Hui C, Joughin E, Nettel-Aguirre A, et al. Comparison of cast materials for the treatment of congenital idiopathic clubfoot using the Ponseti method: a prospective randomized controlled trial. Can J Surg. 2014;57(4):247-253.
- A’Court J, Yassa R, Charalambous CP. Litigation related to casting in Orthopaedics—an analysis of claims against the National Health Service in England. Injury. 2017;48(7):1405-1407.