
Current Concept Review
Pediatric Ankle Syndesmosis Injuries
1California Northstate University College of Medicine, Elk Grove, CA; 2Valley Children’s Hospital, Madera, CA
Correspondence: Jill Friebele, MD, 9300 Valley Children’s Place, Madera, CA 93636, Mailstop FE10. E-mail: [email protected]
Received: July 27, 2022; Accepted: September 26, 2022; Published: November 1, 2022
Volume 4, Number 4, November 2022
Abstract:
Ankle syndesmosis injuries occur in 1% of pediatric ankle trauma. In the younger populations, an open physis has been thought to be a protective factor against syndesmotic injury and therefore favors more Salter-Harris type injuries. Clinical methods used to diagnose syndesmotic injuries may not be effective in the pediatric population. Radiographic findings are mostly based on the study of adolescent and adult populations. Therefore, syndesmotic injuries may be overlooked in the younger pediatric patient with ankle trauma and open physes. Here we present a review of the literature of ankle syndesmotic injuries and demonstrate how isolated injury can be missed in the younger pediatric patient. Further research is needed to fully characterize clinical exam and radiographic findings of syndesmotic injury in the younger pediatric patient and how these may change with time and growth.
Key Concepts
- Diagnosis of ankle syndesmotic injuries, including isolated injuries, in children is difficult and has different criteria for diagnosis than in adults.
- Syndesmotic anatomy changes with growth and false positives or negatives in diagnosis are possible using plain radiographs alone.
- Stress radiographs, bilateral radiographs, and MRI imaging should be considered when clinical suspicion is high.
- Consider tightrope fixation in lieu of syndesmotic screws as recent literature in adolescents supports it as equivalent or superior regarding patient outcomes.
Introduction
Injuries to the ankle syndesmosis comprise up to 5.7% of ankle injuries in the general population and 1% of pediatric ankle trauma.1,2 Incidence of syndesmotic injury in patients under 18 years of age is roughly 1 per 100,000 patient years.3 Children playing certain sports such as hockey, wrestling, and football are susceptible to syndesmotic injury, but injury can occur from other trauma or activities of daily life.2,4,5
Pertinent Anatomy
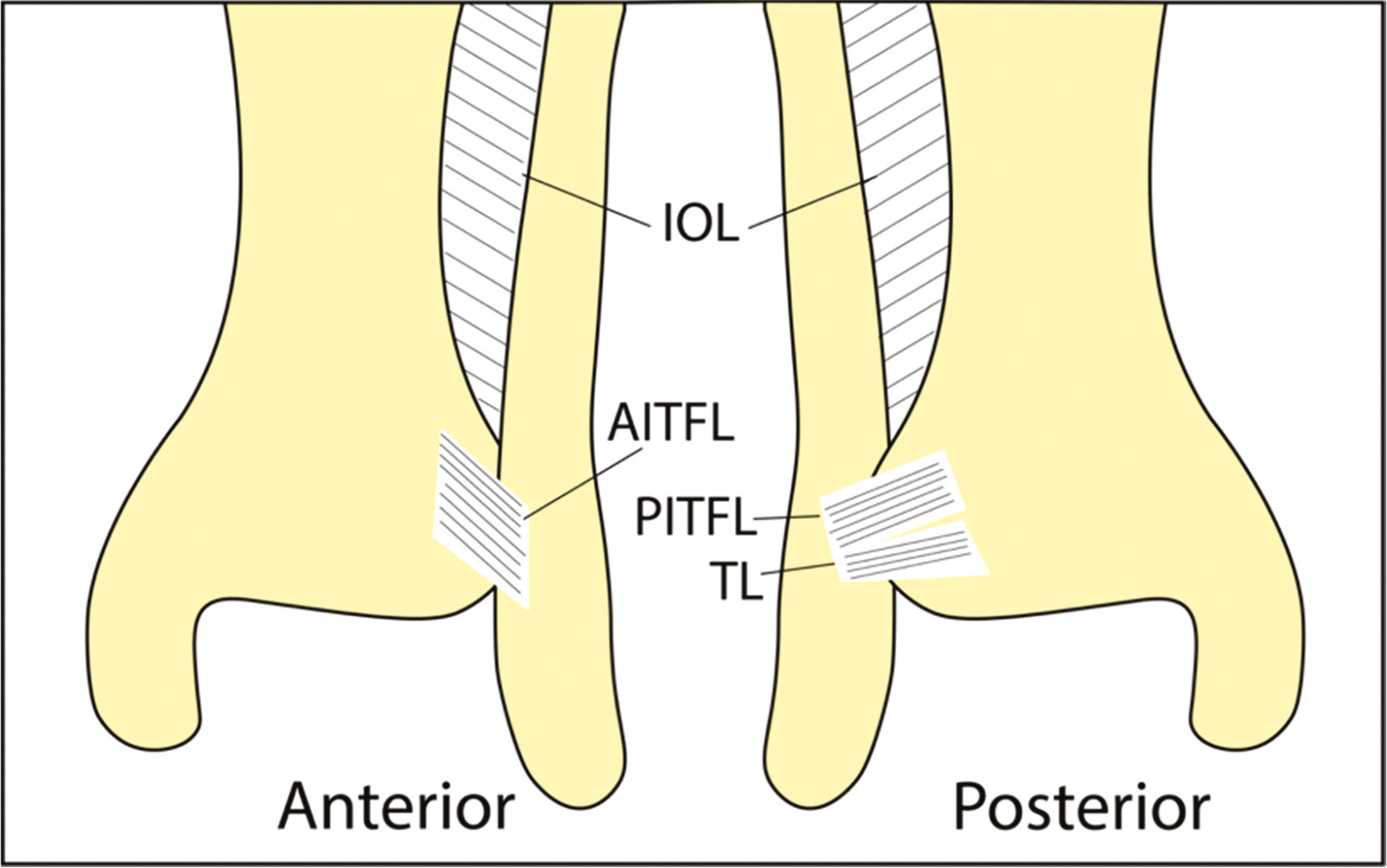
Four ligaments comprise the syndesmotic ankle ligament complex (Figure 1): the anterior inferior tibiofibular ligament (AITFL), commonly injured first; the posterior inferior tibiofibular ligament (PITFL); the transverse ligament; and the interosseus ligament (IOL).6,7 The AITFL provides 35%, the IOL provides 22%, and the combined PITFL and transverse ligament provides 42% of the strength of the syndesmosis.8 Grade I, II, and III injuries include combinations of damage to the AITFL, IOL, and PITFL.9,10 The deltoid ligament and lateral ankle ligaments may or may not be associated with syndesmotic injury.11,12
Figure 1. Anatomy of the syndesmosis. Shown are the interosseus ligament (IOL), anterior inferior tibiofibular ligament (AITFL), posterior inferior tibiofibular ligament (PITFL), and the transverse ligament (TL).
Mechanism of Injury
The mechanism of syndesmotic injury is commonly external rotation of the foot during dorsiflexion.13 Occasionally eversion, which may be associated with damage to the deltoid ligament, and hyper-dorsiflexion are thought to contribute.14 The relationship between the tibia, fibula, and talus in the ankle joint has been well-described, and there are often associated fractures with syndesmotic injury.15 These fractures include Maisonneuve, distal fibular, distal tibial, posterior malleolar, or medial malleolar fractures.2,16
Classification Systems
Distal fibular fractures have been described by the Weber, Lauge-Hansen, and AO/OTA classification systems.17–20 Weber B fractures, roughly equivalent to the Lauge-Hansen supination external rotation classification, may be more common in distal fibula fractures. Weber C fractures are more likely to be associated with injury to the syndesmosis.10,21 Children with open physes can have Salter-Harris fractures in the fibula and tibia; thus, ankle fracture classification systems such as Dias-Tachdjian have been developed for pediatric populations.22–24
An open physis more often leads to certain fractures found in children and is thought to be a protective factor against syndesmotic injury.25 As the physes close, transitional fractures and ligamentous injuries become more likely. This is demonstrated in one study where the youngest children had intraarticular tibial fractures and malleolar fractures (mean ages 10.0 to 11.6), the intermediate aged children had epiphyseal fractures (mean ages 12.4 to 12.9), and the oldest children had avulsion fractures such as Tillaux fractures (mean age 13.1).23 Triplane fractures are possible and may occur in younger patients versus Tillaux fractures.26–28 Chaput’s tubercle fractures and injuries to the subcortical tibial mortise are thought to be transitional injuries between Tillaux fractures and syndesmotic injury in adults.29
The distal fibular physis is associated with Salter-Harris I fractures and closes at approximately 19 years of age.30–32 In addition to several mechanisms described by Dias-Tachdjian, two-plane fractures are associated with Salter-Harris II fractures.23,24 A case of fibular Salter-Harris II fracture has also been described with the impingement of the high ankle.33 The distal tibial physis is associated with Salter-Harris III fractures, commonly presenting as Tillaux fractures, and closes at approximately 15 and 17 years of age in girls and boys, respectively.34 Salter-Harris IV fractures are associated with supination-inversion injuries from the Dias-Tachdjian classification, triplane fractures, Chaput’s tubercle fractures, and injuries to the subcortical tibial mortise.24,26,27,29
Greater tensile strength in ligaments of children may favor fractures, periosteal stripping, osteochondral injuries, and avulsions over sprains.7,35 Therefore, when ligamentous injuries occur in the younger populations, these are more easily missed and can result in poorer outcomes with persistent disability.4,7,34,36
Radiographic and Advanced Imaging Studies
On plain radiographic film, it has been shown that increased tibiofibular clear space (>7 mm) and medial clear space (>5 mm) in the mortise view were highly determinant of surgical intervention.2 Tibiofibular overlap is also used but may be poor at predicting injury.37 These methods can be unreliable and are susceptible to anatomic variability, especially in the pediatric population where syndesmotic anatomy may vary with growth.16,38 It has been theorized in adults that since the anterior talar dome is wider than its posterior aspect, the medial clear space may appear to be artificially enlarged during plantar flexion.39 This may also apply to children in equinus and yield false positives in determining whether the medial clear space is widened. However, this concept may be unclear in children since developmental anatomy is not considered.
A study on radiographic indices in children showed the distribution of medial clear space, tibiofibular clear space, tibiofibular overlap, and superior clear space stratified by age and demonstrated that measurements such as medial clear space may be unreliable until age 8.40 In a study of 48 children, 23% had greater than 6mm of tibiofibular clear space, and overlap appeared as late as 16 years old in boys on the mortise view.41 Another study showed >6 mm tibiofibular clear space and <2 mm tibiofibular overlap were not sensitive and only moderately specific to syndesmotic injury in adolescents.25 Tibiofibular clear space and medial clear space decrease with age, while tibiofibular overlap appears at 6.1 years in AP and 7.9 years in mortise views and increases with age.42 Studies support the use of stress radiographs in diagnosis in addition to bilateral ankle radiographs as there is less than 50% difference of ankle measurements in over 90% of uninjured patients.42,43
Other modalities have good diagnostic capability. Dynamic ultrasound can detect AITFL rupture and has been tested in patients as young as 16 years old.44 CT can be used to optimize treatment and studies have used this method to better understand the anatomy and micromovement of the high ankle joint.45–47 MRI has extremely high sensitivity and specificity in acute syndesmosis injury.48 One retrospective study showed that MRI images in children and adults were similar, except children had more periosteal stripping.49 Another MRI study showed the changes of the syndesmosis with growth.50 Lastly, arthroscopic methods can be employed for direct visualization of the ligaments.51
Treatment
Treatment in pediatric patients includes conservative management as well as surgical methods.6 The goal is ankle joint stability as well as alignment.52 Conservative treatment usually involves immobilization for 3 to 6 weeks to allow ligaments to heal.6 Indications for surgery include concomitant deltoid ligament injury, malleolar fracture, or increased medial clear space. Intraoperative tests include the lateral stress test, also known as the Cotton test, and external rotation stress test.53
Surgical treatment options vary as comparative studies are limited in children and have included reduction and fixation with syndesmotic screws, suture buttons, or even mini-fragment plates with suture.54,55 Syndesmotic screws are angled 30 degrees anteriorly from lateral to medial, are tricortical or quadcortical, and can be removed routinely at 6 or 12 weeks or if symptomatic.6 Postoperative course of suture buttons may be advantageous in children, as these implants typically do not require removal and may allow greater mobility and earlier weight-bearing, but studies are needed in pediatric populations.6,56 In one study, time to return to weight-bearing in a group with syndesmotic surgical fixation was 7.6 weeks.2 In a retrospective study, Lurie et al. compared outcomes of syndesmotic screw versus suture button fixation in 77 eligible adolescents including six patients with immature physes.54 They found that both techniques were similar regarding syndesmotic reduction and functional outcome (Foot and Ankle Ability Measure) on follow up; however, rates of implant removal were higher with syndesmotic screws, possibly because they were electively removed. Again, this study is difficult to extrapolate to the pediatric population given the small numbers of younger patients included in the study. Over the years, we have found that planned removal of screw fixation of the syndesmosis is not always necessary, as the younger pediatric patient population seems to have less incidence of ankle stiffness with screw fixation. However, our preference on syndesmotic fixation has transitioned from screw fixation to more tightrope fixation to avoid the potential ankle stiffness and need for screw removal in the future.
Limitations
Literature on the pediatric diagnosis of syndesmotic injuries and treatment is limited and includes mainly adolescent patient populations. Sensitivities and specificities of direct palpation, the squeeze test, dorsiflexion-external rotation stress test, and hopping test on physical examination have been described, but more studies are needed in pediatric populations.57 When looking at treatment type based on age, algorithms have been developed in order to predict which patients may need operative intervention based on risk factors.2 But again, these are based on retrospective studies. Parameters for surgical intervention in the younger pediatric patient have yet to be established. Studies showing suture button outcomes for children with immature physes are needed.6 Furthermore, determining targets for postoperative outcomes with respect to tibiofibular clear space, tibiofibular overlap, and medial clear space are needed.54
Illustrative Example 1
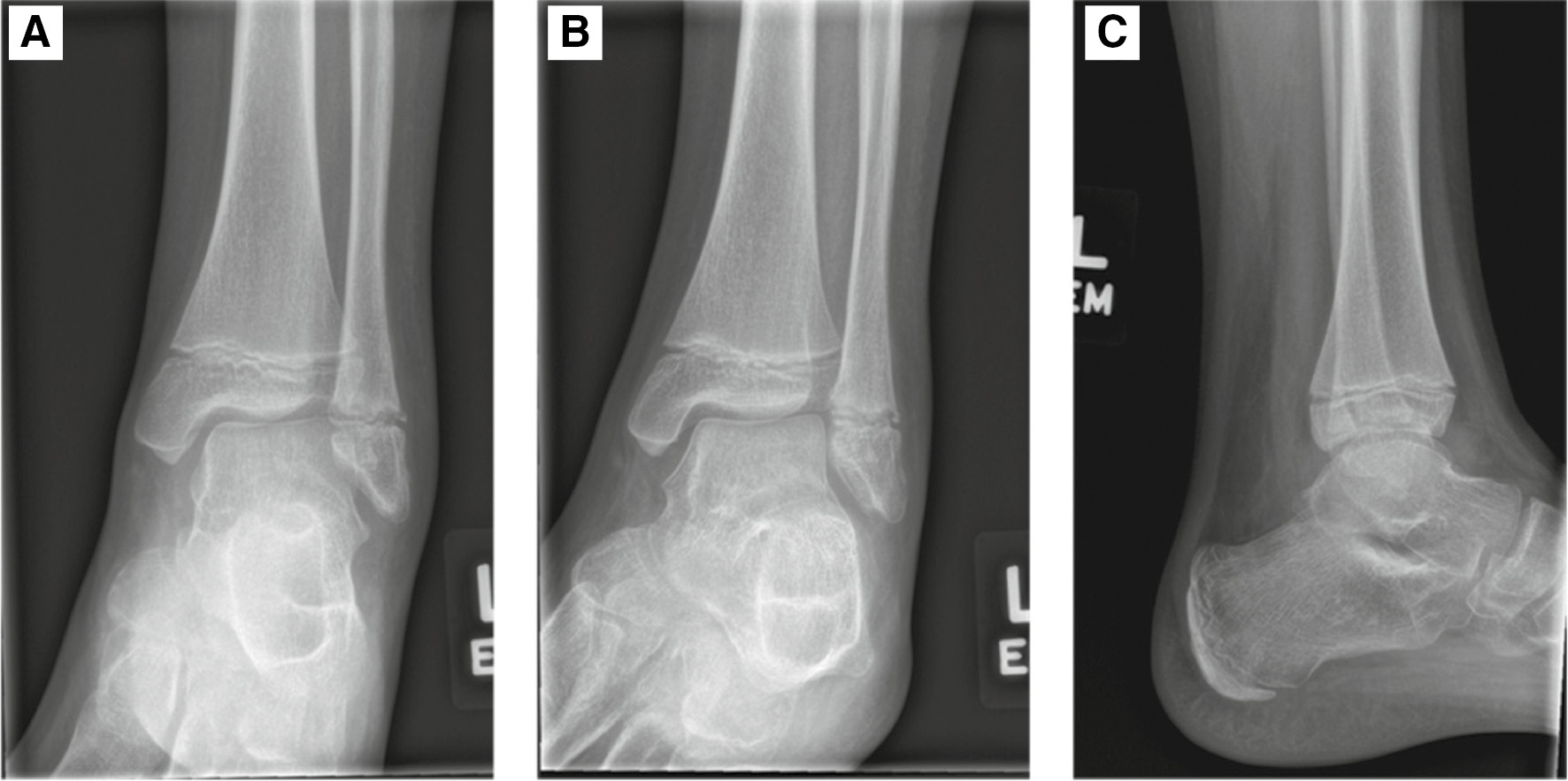
The first case is a young pediatric patient who initially did not have any risk factors suggestive of a syndesmotic injury other than the presence of a fracture. An 11-year-old male with past medical history of mild idiopathic scoliosis came to the Emergency Department with left ankle pain after he was running and jumped off a stump, twisting his ankle earlier the same day. Ankle radiographs showed lateral soft tissue swelling and joint effusion, with a possible buckle of the distal fibular metaphysis seen on the mortise view, but no displaced fractures (Figure 2). Physes were open with possible slight widening of the distal fibular physis medially. Medial clear space measured <5 mm with tibiofibular clear space <7 mm. This was consistent with a Salter-Harris I or II nondisplaced distal fibula fracture. He was seen by orthopaedics and placed in a short leg weight-bearing cast for 4 weeks.
Figure 2. (A) AP radiograph. (B) Mortise view demonstrating acceptable limits for the medial clear space (<5 mm) and tibiofibular clear space (<7 mm). (C) Lateral view.

On follow-up a month later, the cast was removed and radiographs showed decreased soft tissue swelling, some callus formation at the distal fibular physis, and maintenance of the ankle joint alignment (Figure 3). On exam, he still had mild ankle swelling and tenderness to palpation at the distal fibula. He was placed in a walking boot with instructions on ankle range of motion and strengthening exercises.
Figure 3. (A) AP, (B) mortise, and (C) lateral radiographs demonstrating callus formation at the distal fibula and acceptable alignment of the ankle.
The patient returned 1 month later with continued ankle pain radiating proximally and persistent antalgic gait despite being compliant with treatment recommendations. Upon clinical exam, he had ongoing diffuse swelling with tenderness over the distal fibula as well as the AITFL and PITFL. He had a negative squeeze test, but he had lateral pain with external rotation of the foot. Radiographs, including a stress view, showed slight widening of the medial clear space compared to the AP radiograph as well as widening of the tibiofibular clear space with stress (Figure 4). MRI was obtained of the left ankle without contrast and revealed a partial tear or sprain of the AITFL, but the PITFL and other ligaments were intact (Figure 5). There was also a small focus of edema in the lateral talar dome consistent with an osteochondral defect.
Figure 4. (A) AP radiograph of the ankle. (B) Stress view of the ankle demonstrating widening of the medial clear space compared to the AP radiograph and widening of the tibiofibular joint measuring >7 mm.

Figure 5. MRI of the ankle. A) T2 weighted axial image. B) T2 weighted coronal image. C) T1 weighted coronal image. (A,B) Arrows demonstrate signal in the AITFL. (C) Arrow demonstrating sclerotic focus of subchondral osteochondral defect in the lateral talar dome measuring 0.7 cm.

Repair of the left ankle syndesmosis was performed with the ankle syndesmotic suture button (TightRope; Arthrex, Naples, FL). A large bone clamp was placed around the distal fibula and medial malleolus. This reduced the talus and restored tibiofibular overlap. A guidewire was placed from the fibula to the tibia at a 30-degree angle posterior to anterior and 1 cm above the physis. The construct (TightRope; Arthrex) with medial button were passed through the hole and the other end was tied down to the fibula. Final fluoroscopic images showed anatomic alignment. He was made non-weight-bearing with a CAM walker boot for 6 weeks followed by weight-bearing as tolerated with the CAM boot for another 6 weeks.
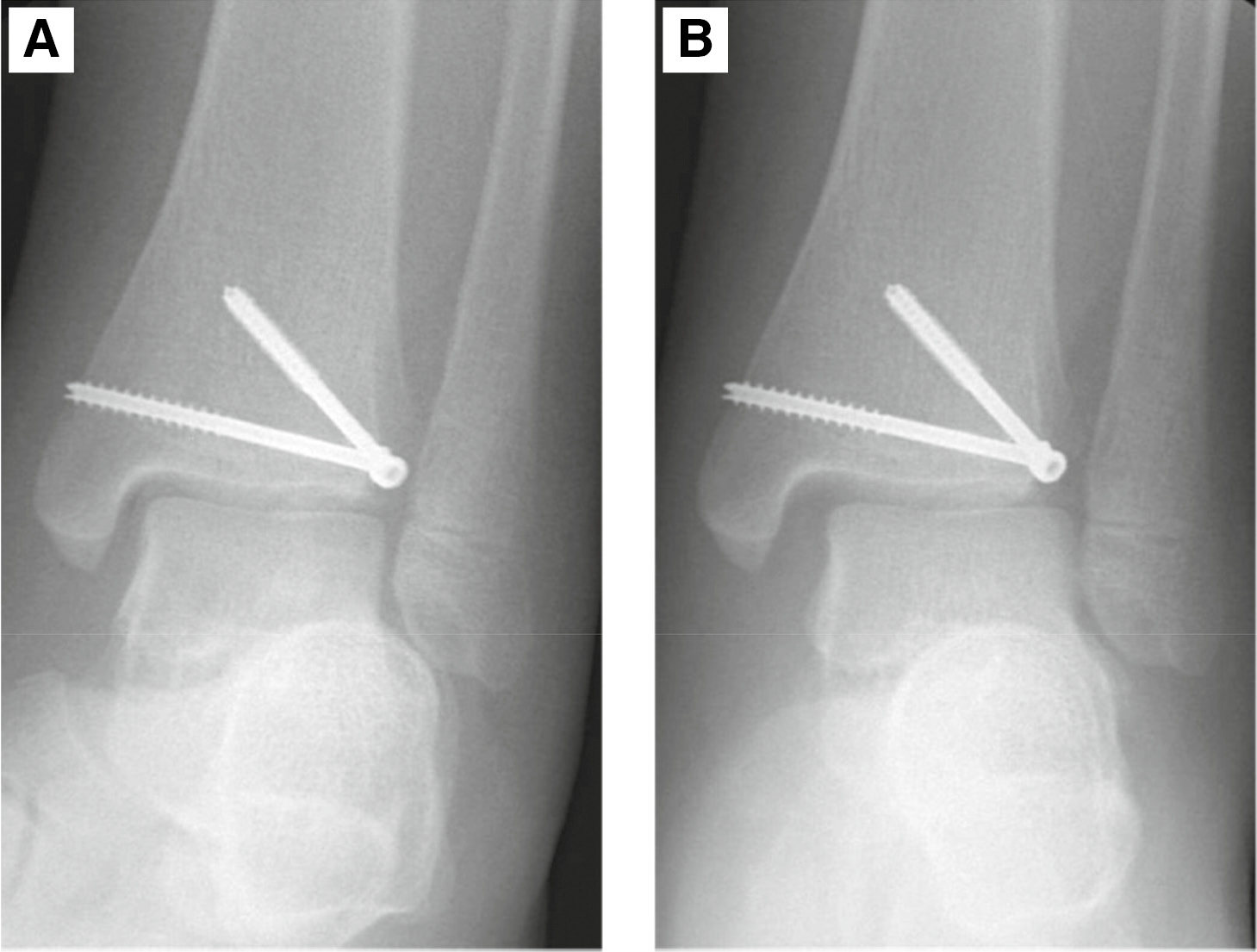
At his 6-week postoperative visit, he had healed well with good passive ankle range of motion. X-ray showed intact suture button without syndesmosis disruption (Figure 6). At the 12-week postoperative visit, he had slight soreness around the ankle with compression. He had full inversion/eversion of the ankle but mild stiffness in flexion and extension. He was able to ambulate with heel-toe gait and was able to hop on one leg. Patient started at-home rehabilitation for strengthening. He was doing well at 9-month follow-up visit and back to regular activities without pain.
Figure 6. (A) Postoperative AP and (B) lateral radiographs of the ankle.

The patient’s young age with open fibular physis and nondisplaced fracture should have been low risk for syndesmotic injury. Even with the syndesmotic injury, he failed to respond to conservative management and eventually required surgical intervention. When it comes to fracture characteristics, in this case, the stresses on bone from the original injury may have made the resultant Salter-Harris type I fracture equivalent to a Weber B fracture. This has been suggested in prior reports of adolescent patients with displaced Salter-Harris I fractures resulting in syndesmotic injuries.30,32 Another study looking at predictive factors for surgical intervention included patients as young as 8.9 years old and demonstrated that an open physis is associated with 5 times lower odds of needing surgical intervention for syndesmosis injury.2 Because of these reasons, our patient had a delay in diagnosis and eventually required operative treatment of the syndesmotic injury.
Illustrative Example 2
The second case illustrates the complicated transition between the skeletally immature and skeletally mature patient. A 15-year-old otherwise healthy male sustained an injury to the left ankle during a fall while roller skating. Ankle radiographs showed a significantly displaced Tillaux fracture with the fragment extruded and completely rotated 90 degrees, with a possible nondisplaced Salter-Harris II distal fibula fracture. Consistent with Tillaux fractures, his physes were starting to close but the transitional fracture theoretically would have been protective of a concomitant syndesmotic injury (Figure 7). He was taken to the operating room and underwent open reduction of the Tillaux fragment and fixation with 4.0 mm cannulated screws. Stress maneuvers were performed intraoperatively with an external rotation stress test, and this showed widening of the medial clear space (Figure 8).
Figure 7. Preoperative (A) AP, (B) mortise, and (C) lateral radiographs showing a displaced and rotated Tillaux fragment with a subtle nondisplaced Salter-Harris II distal fibula fracture.
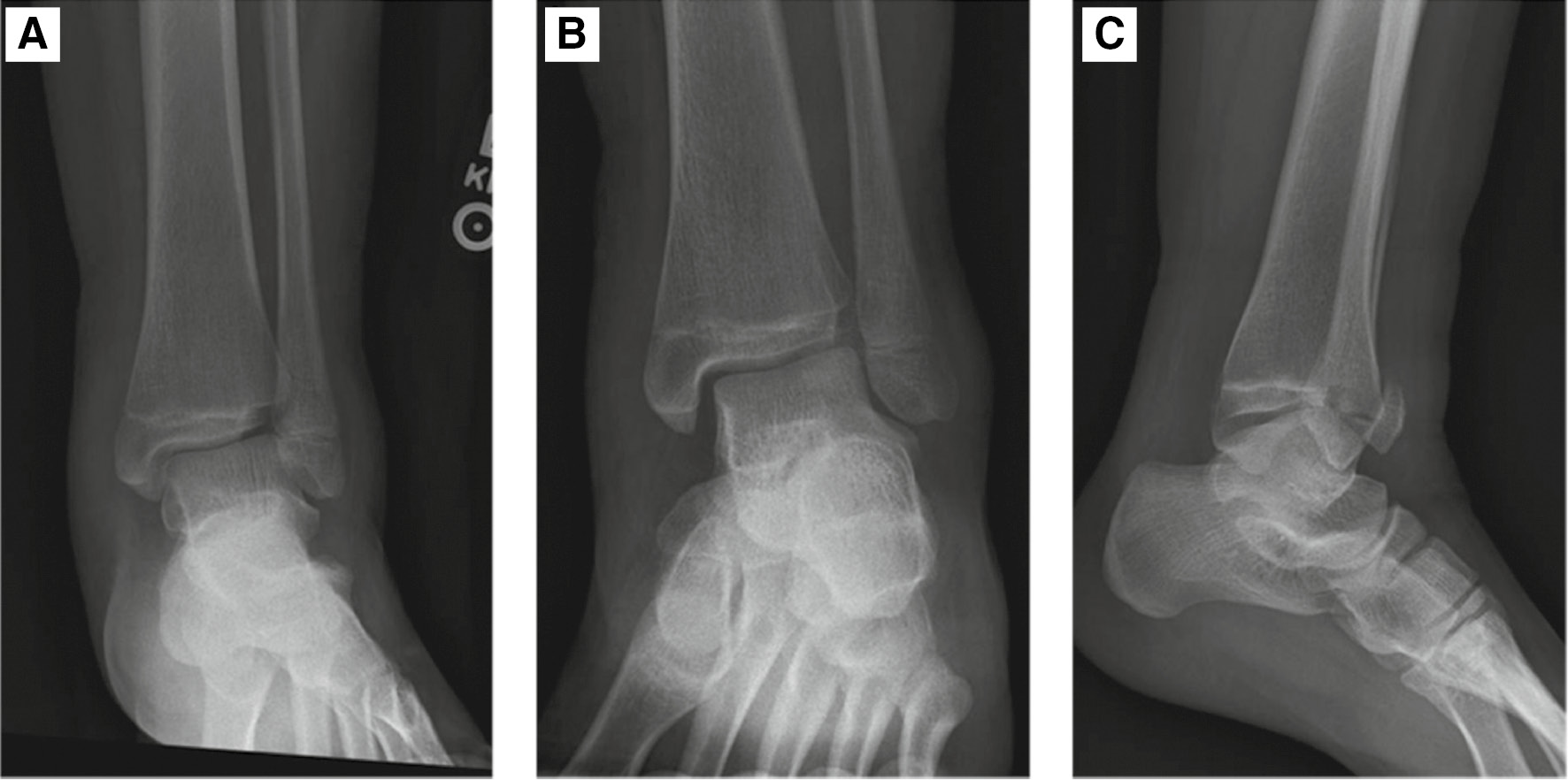
Figure 8. Intraoperative fluoroscopy after fixation of the Tillaux fragment. (A) AP radiograph of the ankle. (B) Stress view of the ankle demonstrating widening of the medial clear space and decreased tibiofibular overlap compared to the AP radiograph.
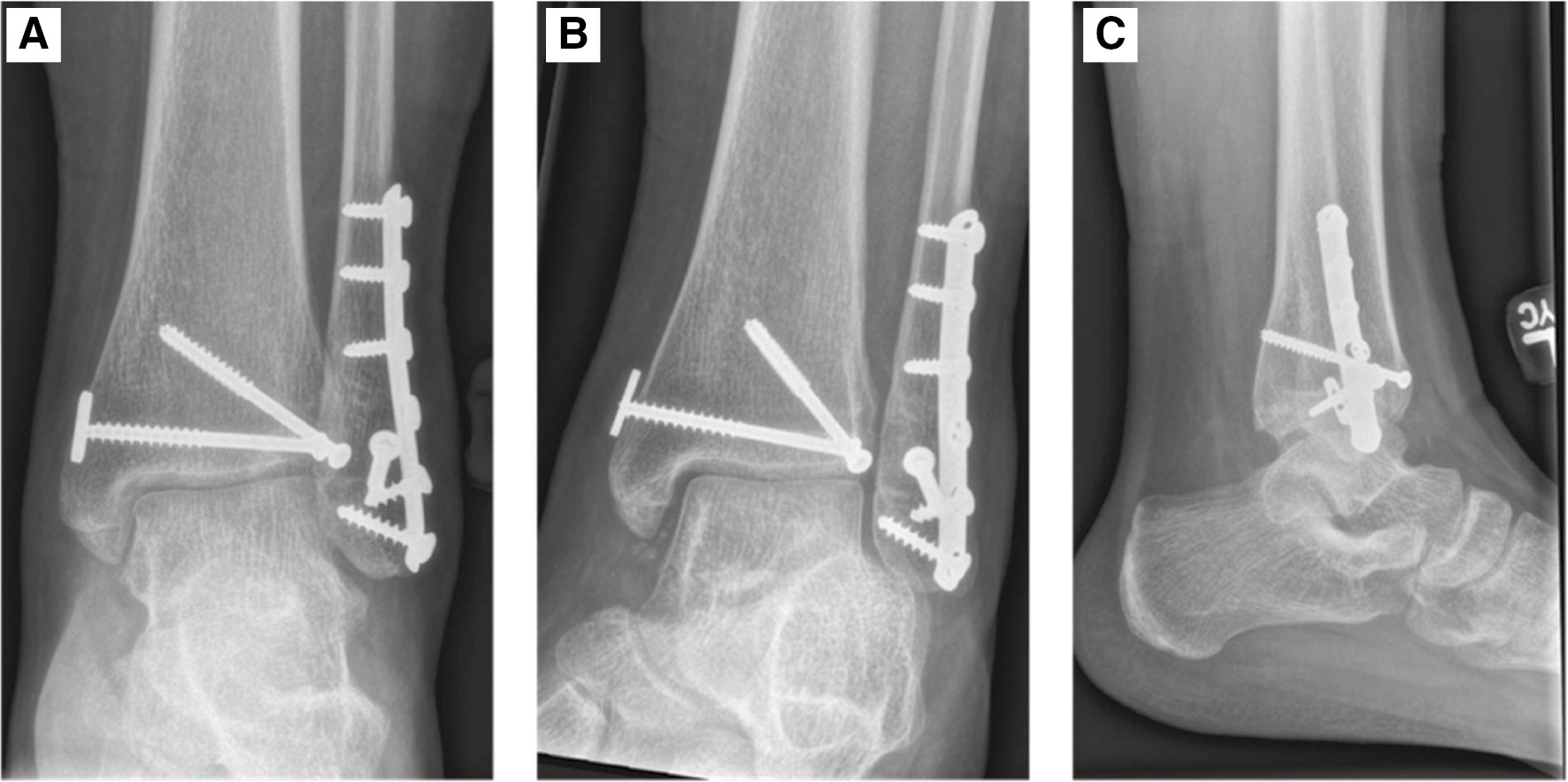
Because of this, we proceeded with fixation of the Salter-Harris II distal fibula fracture. However, repeat external rotation stress test after fibular fixation continued to show widening of the medial clear space and therefore, repair of the ankle syndesmosis was performed with suture button fixation (TightRope; Arthrex) in a similar fashion to the previous case. This reduced the talus, restored tibiofibular overlap, and repeat stress maneuvers demonstrated stabilization of the ankle (Figure 9). Postoperatively, he was placed in a short leg cast and made non-weight-bearing for a total of 6 weeks. At 6 weeks postoperation, he was transitioned to a CAM walker boot with gradual weight-bearing and ankle range of motion exercises. At 3 months, he was pain free with almost symmetric ankle range of motion. He was weaned out of the boot and continued working on strengthening with physical therapy. Radiographs showed anatomic alignment of the ankle with his fractures well healed (Figure 10). This example demonstrates that even in the setting of transitional type fractures, ankle stability should still be assessed and may need to be treated.
Figure 9. Intraoperative fluoroscopy after fibular and suture button fixation. (A) AP radiograph of the ankle. (B) Stress view of the ankle demonstrating no widening of the medial clear space and restored tibiofibular overlap compared to the AP radiograph.
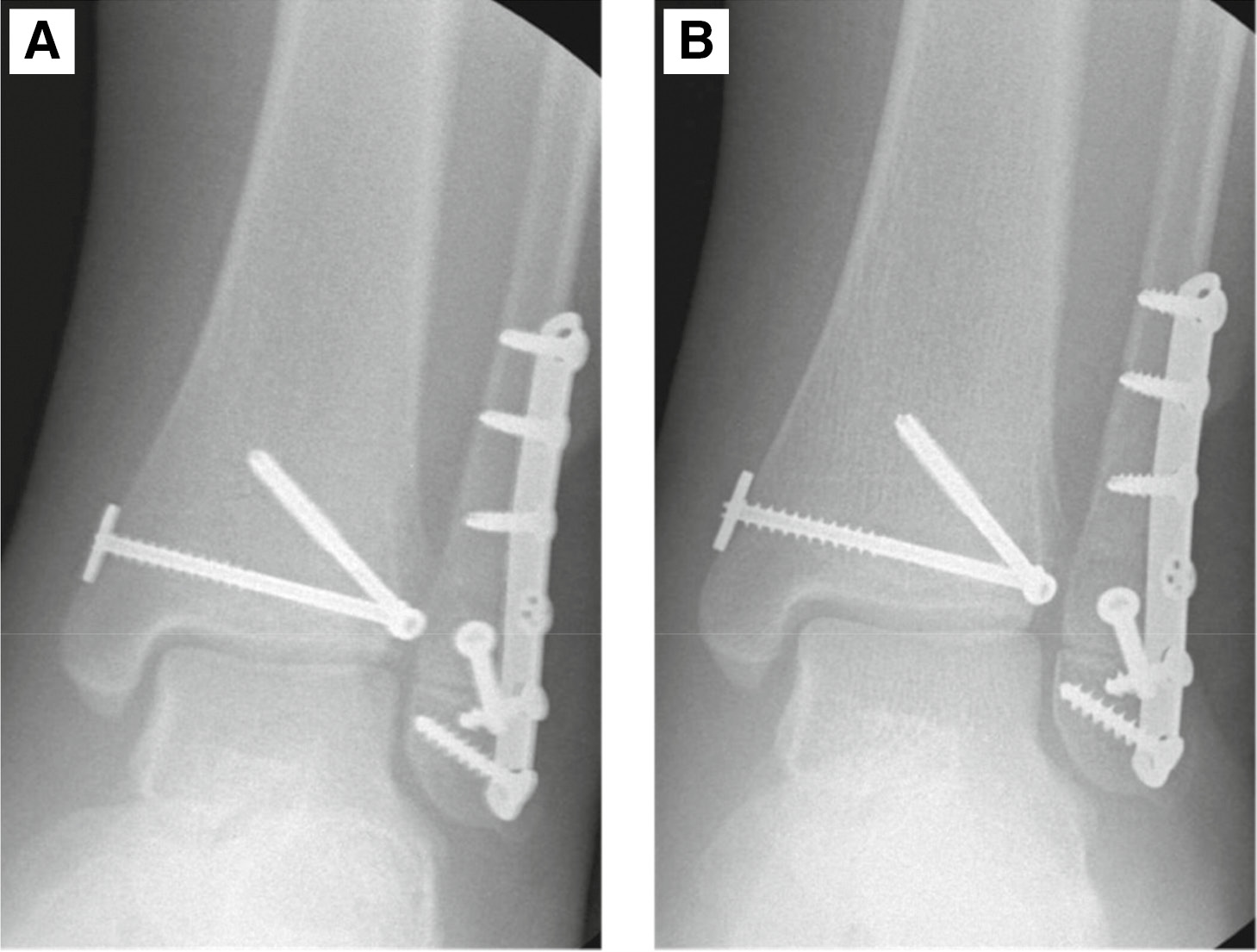
Figure 10. (A) Postoperative AP, (B) mortise, and (C) lateral radiographs of the ankle.
Summary
Previous studies are limited in terms of isolated investigation of the younger pediatric population. For these reasons, it is recommended that syndesmotic injuries be suspected in children of all ages with continuing ankle pain after trauma and conservative management. The diagnosis of syndesmosis injuries is guided by physical examination and can eventually be made by obtaining stress radiographs, bilateral ankle radiographs for comparison, and MRI when pain fails to improve after nonoperative management.
During operative management, suspected ankle syndesmosis injuries can be diagnosed with the Cotton test, external rotation test, comparison films, or even direct visualization. Fixation can utilize screws or suture buttons with adolescent studies showing a mild preference for suture button fixation to avoid the need for future screw removal.
Future studies should focus on changes in the tibiofibular relationship with growth, clinical exam findings that may be unique and helpful in the younger pediatric patient for diagnosing syndesmotic injuries, radiographic factors that may more reliably indicate syndesmotic injuries in the younger pediatric population, and outcomes from using suture buttons for fixation.
Disclaimer
No funding was received for this study. The authors have no conflicts of interest to report.
References
- Fallat L, Grimm DJ, Saracco JA. Sprained ankle syndrome: prevalence and analysis of 639 acute injuries. J Foot Ankle Surg. 1998;37(4):280–285.
- Kramer DE, Cleary MX, Miller PE, et al. Syndesmosis injuries in the pediatric and adolescent athlete: an analysis of risk factors related to operative intervention. J Child Orthop. 2017;11(1):57-63.
- Vosseller JT, Karl JW, Greisberg JK. Incidence of syndesmotic injury. Orthopedics. 2014;37(3):e226-e229.
- Mauntel TC, Wikstrom EA, Roos KG, et al. The epidemiology of high ankle sprains in national collegiate athletic association sports. Am J Sports Med. 2017;45(9):2156-2163.
- Lamer S, Hébert-Davies J, Leduc S, et al. Epidemiology of syndesmotic fixations in a pediatric center: a 12-year retrospective review. Medicine (Baltimore). 2019;98(24):e16061.
- Shore BJ, Kramer DE. Management of syndesmotic ankle injuries in children and adolescents. J Pediatr Orthop. 2016;36(Suppl 1):S11-S14.
- Baldassarre RL, Pathria MN, Huang BK, et al. Periosteal stripping in high ankle sprains: an association with osteonecrosis. Clin Imaging. 2020;67:237-245.
- Ogilvie-Harris DJ, Reed SC. Disruption of the ankle syndesmosis: diagnosis and treatment by arthroscopic surgery. Arthroscopy. 1994;10(5):561-568.
- Molloy A, Selvan D. DeLee & Drez’s Orthopaedic Sports Medicine: Principles and Practice. 4th ed. Philadelphia: Elsevier/Saunders; 2015.
- Qiu HB, Jiang J, Porter D. A new intraoperative syndesmosis instability classification system: utility and medium-term results in closed displaced ankle fractures. Orthop Surg. 2017;9(4):365-371.
- Debieux P, Wajnsztejn A, Mansur NSB. Epidemiology of injuries due to ankle sprain diagnosed in an orthopedic emergency room. Einstein (Sao Paulo). 2020;18:eAO4739.
- Chan KB, Lui TH. Role of ankle arthroscopy in management of acute ankle fracture. Arthroscopy. 2016;32(11):2373-2380.
- Rasmussen O. Stability of the ankle joint. Analysis of the function and traumatology of the ankle ligaments. Acta Orthop Scand Suppl. 1985;211:1-75.
- Hopkinson WJ, St Pierre P, Ryan JB, et al. Syndesmosis sprains of the ankle. Foot Ankle. 1990;10(6):325-330.
- Hermans JJ, Beumer A, de Jong TA, et al. Anatomy of the distal tibiofibular syndesmosis in adults: a pictorial essay with a multimodality approach. J Anat. 2010;217(6):633-645.
- Prada-Canizares A, Auñon-Martin I, Pretell-Mazzini J, et al. Pediatric Maisonneuve: case report of a rare pattern of injury. J Pediatr Orthop B. 2013;22(5):470-474.
- Weber BG. Die Verletzungen des oberen Sprunggelenkes. Aktuelle Probleme in der Chirurgie. 1972;3:103-107.
- Lauge-Hansen N. Fractures of the ankle. II. Combined experimental-surgical and experimental-roentgenologic investigations. Arch Surg. 1950;60(5):957-985.
- Shariff SS, Nathwani DK. Lauge-Hansen classification--a literature review. Injury. 2006;37(9):888-890.
- Spiegel PG. Fracture and dislocation compendium. Orthopaedic trauma association committee for coding and classification. J Orthop Trauma. 1996;10:1-154.
- Kahraman S, Ceylan H, Sönmez M, et al. The ANK nail treatment of lateral malleolar fractures with syndesmosis injury: clinical outcomes at 10 years of follow-up. Ulus Travma Acil Cerrahi Derg. 2019;25(1):75-79.
- Salter RB, Harris WR. Injuries involving the epiphyseal plate. J Bone Joint Surg Am. 1963;45(3):587-622.
- Vahvanen V, Aalto K. Classification of ankle fractures in children. Arch Orthop Trauma Surg. 1980;97(1):1–5.
- Dias LS, Tachdjian MO. Physeal injuries of the ankle in children: classification. Clin Orthop Relat Res. 1978;(136):230-233.
- Lurie BM, Bomar JD, Edmonds EW, et al. Functional outcomes of unstable ankle fractures in adolescents. J Pediatr Orthop. 2020;40(7):e572-e578.
- Singleton TJ, Cobb M. High fibular fracture in association with triplane fracture: reexamining this unique pediatric fracture pattern. J Foot Ankle Surg. 2010;49(5):491-494.
- Healy WA 3rd, Starkweather KD, Meyer J, et al. Triplane fracture associated with a proximal third fibula fracture. Am J Orthop (Belle Mead NJ). 1996;25(6):449-451.
- Egol KA, Koval KJ, Zuckerman JD. Handbook of fractures. Sixth edition. ed. Philadelphia: Wolters Kluwer; 2020.
- Pesl T, Havranek P. Rare injuries to the distal tibiofibular joint in children. Eur J Pediatr Surg. 2006;16(4):255-259.
- Spiegel PG, Cooperman DR, Laros GS. Epiphyseal fractures of the distal ends of the tibia and fibula. A retrospective study of two hundred and thirty-seven cases in children. J Bone Joint Surg Am. 1978;60(8):1046-1050.
- Parikh SN, Wells L, Mehlman CT, et al. Management of fractures in adolescents. J Bone Joint Surg Am. 2010;92(18):2947-2958.
- Korsh J, Adolfsen S. Displaced salter-harris type I distal fibula fractures: two case reports and a review of the literature. J Foot Ankle Surg. 2017;56(4):845-850.
- van Sterkenburg MN, van Bergen CJ, Kerkhoffs GM. Juvenile wakeboarder locks ankle on shore. Knee Surg Sports Traumatol Arthrosc. 2010;18(12):1661-1663.
- Ali Al-Ashhab ME, Mahmoud Mohamed AA. Treatment for displaced Tillaux fractures in adolescent age group. Foot Ankle Surg. 2020;26(3):295-298.
- Brown KW, Morrison WB, Schweitzer ME, et al. MRI findings associated with distal tibiofibular syndesmosis injury. AJR Am J Roentgenol. 2004;182(1):131-136.
- Gerber JP, Williams GN, Scoville CR, et al. Persistent disability associated with ankle sprains: a prospective examination of an athletic population. Foot Ankle Int. 1998;19(10):653-660.
- Shah AS, Kadakia AR, Tan GJ, et al. Radiographic evaluation of the normal distal tibiofibular syndesmosis. Foot Ankle Int. 2012;33(10):870-876.
- Nielson JH, Gardner MJ, Peterson MGE, et al. Radiographic measurements do not predict syndesmotic injury in ankle fractures: an MRI study. Clin Orthop Relat Res. 2005;(436):216-221.
- Saldua NS, Harris JF, LeClere LE, et al. Plantar flexion influences radiographic measurements of the ankle mortise. J Bone Joint Surg Am. 2010;92(4):911-915.
- Lakomkin N, Fabricant PD, Cruz AI Jr, et al. Interrater reliability and age-based normative values for radiographic indices of the ankle syndesmosis in children. JB JS Open Access. 2017;2(1):e0004.
- Bozic KJ, Jaramillo D, DiCanzio J, et al. Radiographic appearance of the normal distal tibiofibular syndesmosis in children. J Pediatr Orthop. 1999;19(1):14-21.
- Sung KH, Kwon SS, Moon SJ, et al. Radiographic evaluation of the normal ankle joint in children and adolescent. J Orthop Sci. 2018;23(4):658-664.
- Ogden JA, McCarthy SM. Radiology of postnatal skeletal development. VIII. Distal tibia and fibula. Skeletal Radiol. 1983;10(4):209-220.
- Mei-Dan O, Kots E, Barchilon V, et al. A dynamic ultrasound examination for the diagnosis of ankle syndesmotic injury in professional athletes: a preliminary study. Am J Sports Med. 2009;37(5):1009-1016.
- Liu Q, Lin B, Guo Z, et al. Shapes of distal tibiofibular syndesmosis are associated with risk of recurrent lateral ankle sprains. Sci Rep. 2017;7(1):6244.
- Del Rio A, Bewsher SM, Roshan-Zamir S, et al. Weightbearing cone-beam computed tomography of acute ankle syndesmosis injuries. J Foot Ankle Surg. 2020;59(2):258-263.
- Mousavian A, Shakoor D, Hafezi-Nejad N, et al. Tibiofibular syndesmosis in asymptomatic ankles: initial kinematic analysis using four-dimensional CT. Clin Radiol. 2019;74(7):571 e1-571 e8.
- Vogl TJ, Hochmuth K, Diebold T, et al. Magnetic resonance imaging in the diagnosis of acute injured distal tibiofibular syndesmosis. Invest Radiol. 1997;32(7):401-409.
- Walter WR, Alaia EF, Samim M, et al. Pediatric versus adult magnetic resonance imaging patterns in acute high ankle sprains. Pediatr Radiol. 2021;51(11):2047-2057.
- Nault ML, Hébert-Davies J, Yen YM, et al. Variation of syndesmosis anatomy with growth. J Pediatr Orthop. 2016;36(4):e41-e44.
- Takao M, Ochi M, Oae K, et al. Diagnosis of a tear of the tibiofibular syndesmosis. The role of arthroscopy of the ankle. J Bone Joint Surg Br. 2003;85(3):324-329.
- Egol KA, Dolan R, Koval KJ. Functional outcome of surgery for fractures of the ankle. A prospective, randomised comparison of management in a cast or a functional brace. J Bone Joint Surg Br. 2000;82(2):246-249.
- Stoffel K, Wysocki D, Baddour E, et al. Comparison of two intraoperative assessment methods for injuries to the ankle syndesmosis. A cadaveric study. J Bone Joint Surg Am. 2009;91(11):2646-2652.
- Lurie BM, Paez CJ, Howitt SR, et al. Suture-button versus screw fixation in adolescent syndesmotic injuries: functional outcomes and maintenance of reduction. J Pediatr Orthop. 2021;41(6):e427-e432.
- Georgiadis AG, Jung EK, North WT, et al. Suture fixation of the syndesmosis using readily available materials. Foot Ankle Int. 2015;36(11):1378-1383.
- Porter DA. Evaluation and treatment of ankle syndesmosis injuries. Instr Course Lect. 2009;58:575-581.
- Sman AD, Hiller CE, Rae K, et al. Diagnostic accuracy of clinical tests for ankle syndesmosis injury. Br J Sports Med. 2015;49(5):323-329.