
Original Research
Plaster versus Ortho-Glass®: Does Initial Splint Material Matter in Pediatric Forearm Fracture Outcomes? A Randomized, Prospective Trial
1University of Utah Department of Orthopaedics, Salt Lake City, UT; 2University of Utah Division of Epidemiology, Salt Lake City, UT
Correspondence: Megan L. Campbell, MD, Department of Orthopaedic Surgery, University of Utah, 590 Wakara Way, Salt Lake City, UT 84108. E-mail: [email protected]
Received: October 3, 2022; Accepted: December 12, 2022; Published: February 1, 2023
Volume 5, Number 1, February 2023
Abstract
Background: Various techniques of non-operative management of pediatric forearm fractures have proven to be successful in avoiding surgical risk and obtaining acceptable outcomes for patients. However, the ability of plaster versus fiberglass splint material to maintain reduction of these fractures has not been compared. Our goal was to determine whether splint material affects the success of non-operative management of pediatric forearm fractures.
Methods: All patients aged 0-18 years with a traumatic forearm fracture requiring reduction were enrolled prospectively and randomized to fiberglass (Ortho-Glass®, Essity Medical Solutions, Charlotte, NC) or plaster sugartong splints. A total of 230 patients met inclusion criteria: 90 randomized to plaster and 140 to fiberglass. Patients were stratified based on location of fracture: distal radius fractures (DRF), middle both bone forearm fractures (BBFFx), and proximal BBFFx. Radiographic outcomes including residual deformity and clinical outcomes including conversion to surgery were evaluated in all patients. Statistical analysis was performed with t-test, Wilcoxon rank sum, Chi-Square, or Fisher’s exact tests where applicable.
Results: Radiographic and clinical outcomes were similar between fiberglass and plaster splints. Overall, only 2.6% of patients required conversion to surgery, 1.1% of the plaster cohort and 3.6% of the fiberglass cohort (p=0.41). No patients required re-reduction with sedation. At final follow-up, 32.5% of middle or proximal BBFFx and 1.3% of DRF healed in “unacceptable” alignment according to classically described guidelines.
Conclusions: There is no difference in the effectiveness of fiberglass or plaster sugartong splints for initial immobilization of pediatric BBFFx and DRF. Rates of conversion to surgery were lower in both groups than previously described. However, there was a trend toward treating “unacceptably” aligned forearm fractures non-operatively and more research is indicated to determine the long-term clinical significance.
Level of Evidence: Level I
Key Concepts
- Splint material is not a contributing factor to maintaining reduction of distal radius and both bone forearm fractures in children.
- Closed reduction and sugartong splinting of pediatric distal radius and both bone forearm fractures provide favorable outcomes with low surgical conversion rate.
Introduction
Forearm fractures are some of the most frequently sustained injuries in the pediatric population. When appropriate, non-operative treatment utilizing closed reduction and immobilization is the recognized standard of care given children’s fracture remodeling capability.1 Non-operative management has proven to be highly successful and avoids risks associated with surgical intervention. Given this, effective initial immobilization to maintain adequate reduction prior to transition to a cast in clinic is vital. Several factors may influence this outcome: adequacy of closed reduction, fracture type and displacement, initial immobilization construct, and splint material.1,2
Many studies have attempted to determine the best type of immobilization to maintain the initial reduction of forearm fractures. Proposed constructs include long and short arm splints/casts; radial gutter, sugartong, and double sugartong splints.3–7 Traditionally, pediatric forearm fractures were immobilized with long arm casts. However, several prospective randomized controlled studies have compared short versus long arm plaster casts and consensus suggests immobilization with below-elbow casts is adequate with fewer complications and less cost overall.3–5
Sugartong splints for initial immobilization have gained popularity given variable success rates of traditional casts, including rates of re-manipulation as high as 91% and increased risk of circumferential constriction of the limb.8 Several studies have demonstrated sugartong splints are effective in maintaining reduction in pediatric forearm fractures. This is the preferred construct at our institution.7,8 However, no clear evidence exists for the best material used for this form of immobilization.
The two most commonly used materials for these constructs are plaster and fiberglass. Proposed benefits to plaster include ease and precision of molding, increased stiffness, low cost, and higher tolerance to swelling.1–3 Proposed benefits to fiberglass include better radiographic visualization, reduced risk of thermal injury, lighter composition, potential for water resistance, and ease of removal.1,2,9 The initial immobilization construct is only the first step of the treatment plan for these fractures; however, to date, the influence of construct material on the ability to maintain an adequate initial reduction in pediatric forearm fractures has not been compared. The purpose of this study was to determine whether plaster or fiberglass sugartong splints are more successful in holding adequate initial reduction in pediatric forearm fractures and thus minimize re-manipulation, surgical intervention, and complications. We hypothesized plaster sugartong splints better maintain reduction and are thus superior to fiberglass splints in all subsequent outcomes.
Methods
IRB approval was obtained to conduct a randomized controlled trial prior to initiation of the study. All pediatric patients who presented to the emergency department of a single level-1 trauma center with a traumatic forearm fracture were consecutively identified. Notably, there was a 4-month pause in enrollment due to COVID-19. Patients were excluded if their fractures did not require reduction, etiology was atraumatic, physes were closed, fractures were open, or if they presented > 1 week post-injury. Patients lost to follow-up prior to evidence of healing on radiographs were also ultimately excluded. Parents/legal guardians were consented prior to reduction by study coordinators and prospectively enrolled in the study.
Patients underwent standard of care orthogonal radiographs followed by routine reduction by orthopaedic residents. Reductions were performed under fluoroscopic guidance and sugartong splints were applied to hold reduction with the elbow flexed to 90 degrees per usual institutional practice. Splint material, either plaster or prefabricated fiberglass (Ortho-Glass, Essity Medical Solutions, Charlotte, NC), was assigned by even (plaster) versus odd days (fiberglass). Orthopaedic residents were reminded by research assistants for which splint material was to be utilized for each patient based on the day, however, adherence to the assignment was not evaluated and may have been influenced by availability of material in the Emergency Department. Post-reduction, post-splint radiographs, or fluoroscopic orthogonal views were obtained on all patients.
Follow-up care was consistent between all patients and treated per institutional standard of care by eight fellowship-trained Pediatric Orthopaedic Surgeons practicing at one institution. At 1-2 weeks after initial reduction, patients returned to clinic where radiographs were obtained to assess for maintenance of reduction and patients were then transitioned to a circumferential, fiberglass cast. The decision of short versus long arm casting at this point was made at the discretion of the treating surgeon. Patients were followed longitudinally until radiographs demonstrated callus formation bridging four cortices, suggesting fracture healing and thus allowing the cast to be removed; this final follow-up typically occurred between 6-8 weeks post-injury. If loss of reduction was seen at any follow-up prior to fracture healing, the patient underwent operative reduction and internal fixation.
Outcomes were evaluated radiographically and clinically. Primary clinical outcome was determined by conversion to surgery at any time point determined by the treating attending physician. Generally, each provider dictated treatment at their discretion based on standardized radiographic parameters as described below in addition to their clinical evaluation.
Radiographic outcomes were evaluated by assessing fracture deformity at initial presentation, post-reduction, and initial and final follow-up visits. Retrospective radiographic review was performed and several parameters were measured at each time point: angulation and translation in both the sagittal and coronal planes. Translation was recorded as a categorical variable by percent translation across fracture, stratified into quartiles. All fractures were subsequently categorized as “acceptable” if they fell within standardized parameters for the child’s age group according to previously published guidelines. For the purpose of this study, “acceptable” was defined as any displacement, less than 15 degrees of angulation in children under 9 years of age or less than 10–15 degrees in children 9 years or older.1
Patient demographics and fracture characteristics were summarized and stratified by splint material. Continuous variables were summarized using mean (standard deviation/SD), median (inter quartile range/IQR), and range, and compared between groups using t-tests and Wilcoxon rank sum tests. Categorical variables were described as frequency and percentage and compared between groups using Chi-squared tests or Fisher’s exact tests.
Residual deformity at final follow-up was compared to patient and fracture characteristics in the BBFF group using univariable and multivariable logistic regression. Odds ratios were reported with 95% confidence intervals and p-values. Interrater reliability for each radiographic measure was evaluated using data from 40 subjects chosen at random per standard protocol and were assessed by four independent orthopaedic surgery residents with multiple years of training.10 Intraclass correlation coefficient (ICC) values with 95% CI lower bounds less than 0.5, between 0.5 and 0.75, between 0.75 and 0.9, and greater than 0.90 are indicative of poor, moderate, good, and excellent reliability, respectively. All analyses were conducted in R v4.0 (Vienna, Austria). Statistical significance was assessed at the 0.05 level and all tests were two-sided.
A priori power analysis was conducted and considering a fiberglass splint group rate of 30% as non-inferior to the plaster group (at a failure rate of 15%), this would require 224 subjects to achieve 80% power to detect a difference. Thus, when defining “failure” as requirement for surgical intervention or rereduction, a minimum of 224 or more fractures would statistically provide adequate power to detect a 15% absolute difference.
Results
Enrollment was conducted from January 1, 2019, to January 1, 2021, during which 421 patients were eligible for inclusion (Figure 1). Of those, 220 patients were included in the study with a total of 230 forearm fractures; 13 patients were excluded for lack of follow-up or radiographs. Average age at presentation was 9 years old and 34% were female (Table 1). Thirty-four percent of fractures sustained were isolated DRF, 24% were middle BBFFx, and 42% were distal BBFFx. Five patients had bilateral injuries and five were a re-fracture of a previous injury. Ninety fractures were splinted using plaster (39%). Both groups were transitioned to a circumferential, fiberglass cast in clinic at a median of 8.0 days (Table 1). Average follow-up for all patients was 50.3 days (range 22-220).
Figure 1. Trial flowsheet of eligible patients included and final randomization.

Table 1. Patient and Fracture Characteristics Stratified by Splint Type
| Variable | Plaster (N=90) | Fiber glass (N=140) | P-value |
|---|---|---|---|
| Age at Presentation - Mean (SD) | 9.0 (3.5) | 8.9 (3.4) | 0.84a |
| Median (IQR) | 8.6 (6.4, 11.5) | 8.4 (6.2, 11.5) | - |
| Range | (1.8, 17.8) | (2.0, 16.2) | - |
| Gender-Female | 32 (35.6%) | 43 (30.7%) | 0.44b |
| BMI - Mean (SD) | 17.7 (3.2) | 18.0 (4.0) | - |
| Median (IQR) | 16.8 (15.5, 19.0) | 16.8 (15.4, 19.0) | 0.94c |
| Range | (13.6, 29.6) | (13.2, 31.4) | - |
| BMI percentile - Mean (SD) | 57.1 (29.2) | 55.5 (30.1) | - |
| Median (IQR) | 59.6 (30.2, 81.9) | 52.1 (34.8, 80.7) | 0.74c |
| Range | (0.3, 98.4) | (0.2, 99.6) | - |
| Time From Fx to cast - Mean (SD) | 8.4 (2.6) | 7.9 (1.6) | - |
| Median (IQR) | 8.0 (7.0, 9.0) | 8.0 (7.0, 9.0) | 0.92c |
| Range | (5.0, 23.0) | (3.0, 12.0) | - |
| Fracture location - Mid 1/3 BBFF | 23 (25.6%) | 31 (22.1%) | 0.08b |
| Distal 1/3 BBFF | 44 (48.9%) | 53 (37.9%) | - |
| DR | 23 (25.6%) | 56 (40%) | - |
| Pre Reduction Sag Ang - Mean (SD) | 21.7 (12.6) | 22.7 (12.1) | - |
| Median (IQR) | 20.8 (13.7, 26.5) | 21.2 (14.6, 31.1) | 0.45c |
| Range | (0.2, 57.8) | (0.0, 58.3) | - |
| Pre Reduction Cor Ang - Mean (SD) | 10.4 (9.2) | 9.5 (8.4) | - |
| Median (IQR) | 7.2 (3.8, 14.6) | 7.9 (2.9, 13.3) | 0.51c |
| Range | (0.0, 49.2) | (0.0, 48.8) | - |
| Pre Reduction Sag Trans - 0% | 29 (32.2%) | 32 (22.9%) | 0.17b |
| 0-25% | 21 (23.3%) | 39 (27.9%) | - |
| 25~50% | 4 (4.4%) | 19 (13.6%) | - |
| 50~75% | 9 (10%) | 13 (9.3%) | - |
| 75~100% | 13 (14.4%) | 14 (10%) | - |
| >100% | 14 (15.6%) | 23 (16.4%) | - |
| Pre Reduction Cor Trans - 0% | 35 (38.9%) | 42 (30%) | 0.11d |
| 0-25% | 29 (32.2%) | 66 (47.1%) | - |
| 25~50% | 11 (12.2%) | 12 (8.6%) | - |
| 50~75% | 6 (6.7%) | 14 (10%) | - |
| 75~100% | 6 (6.7%) | 3 (2.1%) | - |
| >100% | 3 (3.3%) | 3 (2.1%) | - |
| Post Reduction Sag Angulation - Mean (SD) | 4.7 (3.4) | 4.2 (3.1) | - |
| Median (IQR) | 4.3 (1.7, 7.0) | 3.5 (2.0, 5.9) | 0.33c |
| Range | (0.3, 14.6) | (0.1, 14.1) | - |
| Post Reduction Cor Angulation - Mean (SD) | 3.6 (3.1) | 3.3 (2.8) | - |
| Median (IQR) | 2.7 (1.1, 4.9) | 2.5 (1.3, 4.8) | 0.73c |
| Range | (0.0, 12.9) | (0.0, 15.0) | - |
| Post Reduction Sag Trans - 0% | 42 (46.7%) | 74 (52.9%) | 0.58d |
| 0-25% | 39 (43.3%) | 55 (39.3%) | - |
| 25~50% | 7 (7.8%) | 8 (5.7%) | - |
| 50~75% | 2 (2.2%) | 1 (0.7%) | - |
| 75~100% | 0 (0%) | 2 (1.4%) | - |
| Post Reduction Cor Trans - 0% | 43 (47.8%) | 70 (50%) | 0.89d |
| 0-25% | 39 (43.3%) | 59 (42.1%) | - |
| 25~50% | 6 (6.7%) | 9 (6.4%) | - |
| 50~75% | 1 (1.1%) | 2 (1.4%) | - |
| 75~100% | 1 (1.1%) | 0 (0%) | - |
| Days between reduction to first follow up - Mean (SD) | 8.4 (2.6) | 7.9 (1.6) | - |
| Median (IQR) | 8.0 (7.0, 9.0) | 8.0 (7.0, 9.0) | 0.92c |
| Range | (5.0, 23.0) | (3.0, 12.0) | - |
| Days between reduction to final follow up - Mean (SD) | 54.9 (25.1) | 49.9 (14.6) | - |
| Median (IQR) | 50.0 (44.2, 57.8) | 49.0 (40.0, 55.0) | 0.17c |
| Range | (27.0, 220.0) | (22.0, 131.0) | - |
Missing values: BMI=4, BMI percentile=4.
aT-test, bChi-squared test, cWilcoxon rank sum test, dFisher’s exact test.
Overall, 97% of fractures were treated with closed treatment alone. One patient required wedging of their cast in clinic. No patients required a repeat closed reduction under sedation. One patient was reported to have skin irritation/breakdown from the cast; however, this healed without intervention or complication. When stratified by splint material, no radiographic or clinical outcomes showed a statistically significant difference between groups (Table 2). Six fractures required surgical intervention: one initially splinted with plaster and five initially splinted with fiberglass (p=.41). The decision to convert to surgery was made within 2 weeks of the initial reduction in 5/6 of these patients as beyond 2 weeks, the fracture begins to unite and open reduction and fixation becomes exceedingly more difficult. All fractures requiring surgery were BBFF; no DRF required surgery. No patients required re-reduction at their first follow-up visit. At final follow-up, 1.8% of DRF and 32.5% of BBFF healed in unacceptable alignment (Table 2).
Table 2. Summary of Outcomes Stratified by Splint Type
| Variable | Plaster (N=90) | Fiber glass (N=140) | P-value |
|---|---|---|---|
| 1st Follow up Sag Angulation - Mean (SD) | 7.1 (4.8) | 7.4 (6.1) | - |
| Median (IQR) | 6.0 (3.0, 10.0) | 6.0 (3.0, 10.0) | 0.72a |
| Range | (0.0, 20.0) | (0.0, 30.0) | - |
| 1st follow up Cor angulation - Mean (SD) | 4.2 (3.7) | 3.8 (3.4) | - |
| Median (IQR) | 3.0 (1.0, 6.0) | 3.0 (1.0, 6.0) | 0.40a |
| Range | (0.0, 16.0) | (0.0, 16.0) | - |
| 1st follow up Sag trans - 0% | 28 (31.1%) | 28 (20%) | 0.24b |
| 0-25% | 41 (45.6%) | 75 (53.6%) | - |
| 25~50% | 11 (12.2%) | 25 (17.9%) | - |
| 50~75% | 8 (8.9%) | 8 (5.7%) | - |
| 75~100% | 2 (2.2%) | 4 (2.9%) | - |
| 1st follow up Cor trans - 0% | 41 (45.6%) | 62 (44.3%) | 0.81b |
| 0-25% | 36 (40%) | 58 (41.4%) | - |
| 25~50% | 5 (5.6%) | 12 (8.6%) | - |
| 50~75% | 6 (6.7%) | 6 (4.3%) | - |
| 75~100% | 2 (2.2%) | 2 (1.4%) | - |
| Last Follow up Sag Angulation - Mean (SD) | 8.2 (5.9) | 8.8 (6.8) | - |
| Median (IQR) | 8.0 (3.2, 12.0) | 8.0 (3.0, 14.0) | 0.65a |
| Range | (0.0, 24.0) | (0.0, 29.0) | - |
| Last follow up Cor angulation - Mean (SD) | 5.1 (4.4) | 4.7 (4.8) | - |
| Median (IQR) | 4.0 (2.0, 7.0) | 3.0 (1.0, 7.0) | 0.21a |
| Range | (0.0, 20.0) | (0.0, 26.0) | - |
| Last follow up Sag trans - 0% | 41 (45.6%) | 51 (36.4%) | 0.32b |
| 0-25% | 34 (37.8%) | 67 (47.9%) | - |
| 25~50% | 9 (10%) | 17 (12.1%) | - |
| 50~75% | 5 (5.6%) | 3 (2.1%) | - |
| 75~100% | 1 (1.1%) | 2 (1.4%) | - |
| Last follow up Cor trans - 0% | 53 (58.9%) | 86 (61.4%) | 0.79b |
| 0-25% | 28 (31.1%) | 38 (27.1%) | - |
| 25~50% | 6 (6.7%) | 12 (8.6%) | - |
| 50~75% | 1 (1.1%) | 3 (2.1%) | - |
| 75~100% | 2 (2.2%) | 1 (0.7%) | - |
| Conversion to surgery | 1 (1.1%) | 5 (3.6%) | 0.41b |
| Acceptable BBFF | 49 (73.1%) | 64 (76.2%) | 0.67c |
| Acceptable DR | 23 (100%) | 55 (98.2%) | 1.00b |
| Acceptable Overall | 72 (80%) | 119 (85%) | 0.32c |
aWilcoxon rank sum test, bFisher’s exact test, cChi-squared test.
Given the small number of unacceptably healed DRF (1/78), no further statistical analysis was performed on this group. There was no significant difference in the proportion of BBFF healed in acceptable alignment between those splinted using plaster versus fiberglass, both before and after controlling for baseline patient differences (Figure 2; OR 1.05, p=0.90). However, when comparing patients in a univariate analysis evaluating final alignment parameters regardless of splint material, the average age of patients who healed within acceptable range was 7.8 (SD 3.1) compared to 9 (SD 3.3) who healed outside of acceptable range (p=0.045; Table 3). Age did not remain a significant predictor for final acceptable fracture alignment in our multivariate analysis when controlling for baseline patient differences (Figure 2; OR 0.92). Gender, BMI, and time to cast placement did not have a statistically significant effect on final fracture alignment.
Figure 2. Selected odds ratios for likelihood of final acceptable fracture alignment.
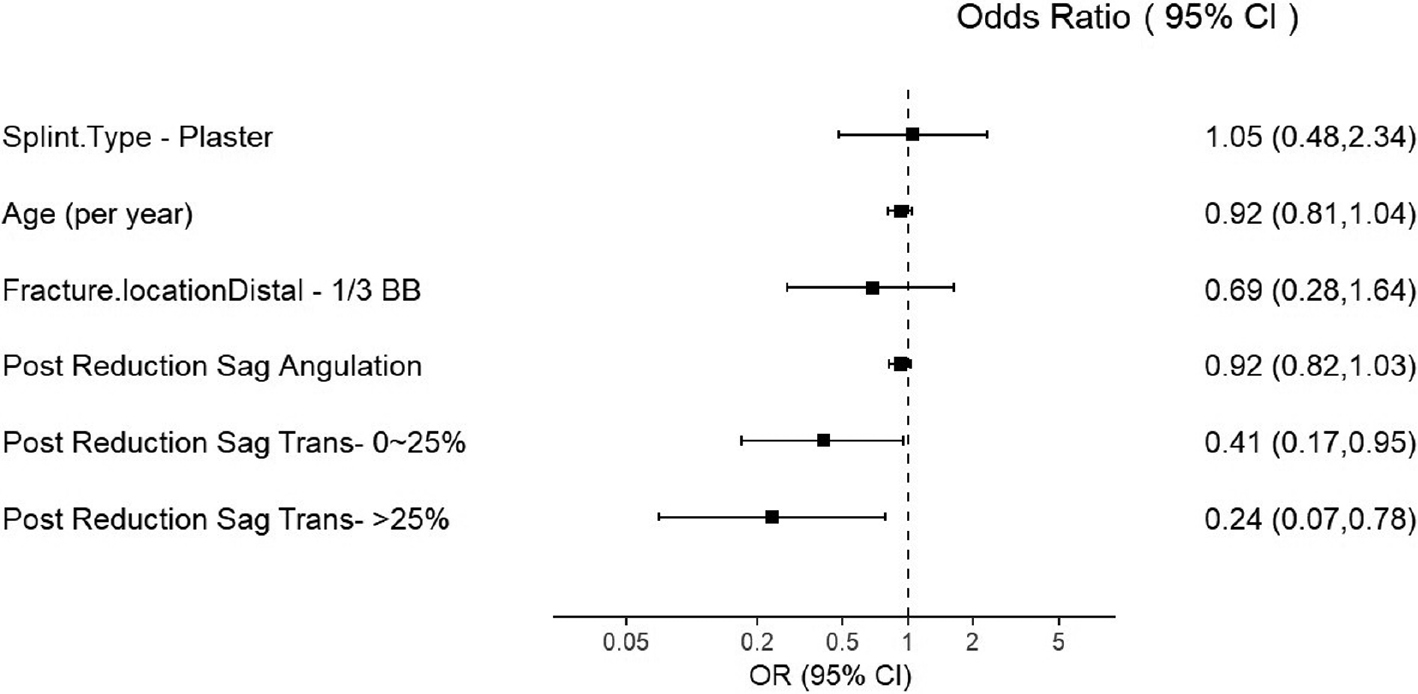
Table 3. Univariable & Multivariable Analysis of Acceptable Final Healing for the BBFF Group
| Variables | ORa (95% CI) | P value | ORb (95% CI) | P value |
|---|---|---|---|---|
| Splint.Type - Plaster | 0.85 (0.41,1.79) | 0.67 | 1.05 (0.48,2.34) | 0.90 |
| Age | 0.89 (0.79,0.99) | 0.038 | 0.92 (0.81,1.04) | 0.19 |
| Female vs. Male | 1.19 (0.55,2.67) | 0.67 | - | - |
| BMI% | 1.00 (0.99,1.01) | 0.88 | - | - |
| Time.From.Fx.to.cast | 1.10 (0.89,1.41) | 0.39 | - | - |
| Fracture.locationDistal - 1/3 BBFF | 0.78 (0.35,1.68) | 0.53 | 0.69 (0.28,1.64) | 0.41 |
| Pre Reduction Sag Angulation | 1.04 (1.01,1.07) | 0.022 | - | - |
| Pre Reduction Cor Angulation | 1.01 (0.96,1.06) | 0.82 | - | - |
| Pre Reduction Sag Trans-0~25% | 0.65 (0.21,1.98) | 0.45 | - | - |
| Pre Reduction Sag Trans ->25% | 0.20 (0.07,0.50) | 0.001 | - | - |
| Pre Reduction Cor Trans-0~25% | 0.57 (0.22,1.42) | 0.23 | - | - |
| Pre Reduction Cor Trans->25% | 0.23 (0.09,0.60) | 0.003 | - | - |
| Post Reduction Sag Angulation | 0.94 (0.84,1.04) | 0.23 | 0.92 (0.82,1.03) | 0.16 |
| Post Reduction Cor Angulation | 1.04 (0.92,1.21) | 0.53 | - | - |
| Post Reduction Sag Trans-0~25% | 0.41 (0.17,0.92) | 0.034 | 0.41 (0.17,0.95) | 0.040 |
| Post Reduction Sag Trans->25% | 0.23 (0.08,0.72) | 0.011 | 0.24 (0.07,0.78) | 0.018 |
| Post Reduction Cor Trans-0~25% | 0.26 (0.11,0.61) | 0.003 | - | - |
| Post Reduction Cor Trans->25% | 0.23 (0.07,0.75) | 0.014 | - | - |
| Days between fix to final follow up | 0.99 (0.97,1.00) | 0.10 | - | - |
aUnivariable models. bMultivariable models.
Several radiographic characteristics were associated with unacceptable final alignment after BBFF (Table 4). Initial fracture translation and sagittal-plane displacement were more likely to produce an unacceptable alignment. Higher post-reduction sagittal translation was also associated with higher odds of healing in unacceptable alignment but was not associated with higher risk of surgery (Table 3). Appreciable translation in the sagittal plane of 0-25% of fracture width increased the odds of final unacceptable healing by 59%, and translation > 25% increased the odds by 76% compared with negligible translation (OR = 0.41 and 0.24, respectively). Residual displacement in the coronal plane after reduction also increased the odds of unacceptable final alignment.
Table 4. Patient and Fracture Characteristics Stratified by Final Healed BBFF Parameters
| Variable | BBFF Acceptable (N=113) | BBFF Unacceptable (N=38) | P-value |
|---|---|---|---|
| Age at Presentation - Mean (SD) | 7.8 (3.1) | 9.0 (3.3) | 0.045a |
| Median (IQR) | 7.1 (5.8, 9.3) | 8.2 (6.5, 11.7) | - |
| Range | (1.8, 15.2) | (2.1, 15.9) | - |
| Gender-Female | 40 (35.4%) | 12 (31.6%) | 0.67b |
| BMI - Mean (SD) | 17.0 (3.3) | 17.4 (2.8) | - |
| Median (IQR) | 15.9 (15.0, 17.9) | 17.0 (15.6, 18.2) | 0.09c |
| Range | (13.2, 31.1) | (13.4, 28.9) | - |
| BMI percentile - Mean (SD) | 53.7 (28.7) | 54.5 (29.7) | - |
| Median (IQR) | 52.2 (34.0, 78.7) | 51.6 (28.4, 83.0) | 0.91c |
| Range | (0.3, 99.6) | (0.2, 97.9) | - |
| Time From Fx to cast - Mean (SD) | 8.1 (1.9) | 7.8 (1.7) | - |
| Median (IQR) | 8.0 (7.0, 9.0) | 7.0 (7.0, 9.0) | 0.49c |
| Range | (5.0, 17.0) | (3.0, 13.0) | - |
| Fracture location - Mid 1/3 BBFF | 42 (37.2%) | 12 (31.6%) | 0.53b |
| Distal 1/3 BBFF | 71 (62.8%) | 26 (68.4%) | - |
| Pre Reduction Sag Ang - Mean (SD) | 25.1 (12.7) | 19.5 (12.5) | - |
| Median (IQR) | 23.5 (16.3, 34.1) | 17.6 (9.5, 26.5) | 0.016c |
| Range | (0.0, 58.3) | (1.8, 53.8) | - |
| Pre Reduction Cor Ang - Mean (SD) | 9.7 (8.1) | 9.3 (7.8) | - |
| Median (IQR) | 7.8 (3.1, 13.1) | 8.7 (2.9, 12.6) | 0.79c |
| Range | (0.2, 42.5) | (0.2, 30.9) | - |
| Pre Reduction Sag Trans - 0% | 47 (41.6%) | 7 (18.4%) | 0.004d |
| 0-25% | 35 (31%) | 8 (21.1%) | - |
| 25~50% | 4 (3.5%) | 4 (10.5%) | - |
| 50~75% | 6 (5.3%) | 2 (5.3%) | - |
| 75~100% | 9 (8%) | 5 (13.2%) | - |
| >100% | 12 (10.6%) | 12 (31.6%) | - |
| Pre Reduction Cor Trans - 0% | 54 (47.8%) | 10 (26.3%) | 0.036d |
| 0-25% | 40 (35.4%) | 13 (34.2%) | - |
| 25~50% | 8 (7.1%) | 5 (13.2%) | - |
| 50~75% | 6 (5.3%) | 4 (10.5%) | - |
| 75~100% | 3 (2.7%) | 4 (10.5%) | - |
| >100% | 2 (1.8%) | 2 (5.3%) | - |
| Post Reduction Sag Angulation - Mean (SD) | 4.4 (3.4) | 5.2 (3.4) | - |
| Median (IQR) | 3.5 (1.6, 6.3) | 5.4 (2.1, 7.1) | 0.18c |
| Range | (0.1, 14.6) | (0.7, 14.1) | - |
| Post Reduction Cor Angulation - Mean (SD) | 3.8 (2.8) | 3.5 (2.8) | - |
| Median (IQR) | 3.1 (1.5, 5.4) | 3.0 (1.5, 5.4) | 0.57c |
| Range | (0.0, 11.5) | (0.1, 14.2) | - |
| Post Reduction Sag Trans - 0% | 64 (56.6%) | 12 (31.6%) | 0.031d |
| 0-25% | 39 (34.5%) | 18 (47.4%) | - |
| 25~50% | 7 (6.2%) | 6 (15.8%) | - |
| 50~75% | 2 (1.8%) | 1 (2.6%) | - |
| 75~100% | 1 (0.9%) | 1 (2.6%) | - |
| Post Reduction Cor Trans - 0% | 62 (54.9%) | 9 (23.7%) | 0.003d |
| 0-25% | 40 (35.4%) | 22 (57.9%) | - |
| 25~50% | 9 (8%) | 5 (13.2%) | - |
| 50~75% | 2 (1.8%) | 1 (2.6%) | - |
| 75~100% | 0 (0%) | 1 (2.6%) | - |
| Days between Fix to first follow up - Mean (SD) | 8.1 (1.9) | 7.8 (1.7) | - |
| Median (IQR) | 8.0 (7.0, 9.0) | 7.0 (7.0, 9.0) | 0.49c |
| Range | (5.0, 17.0) | (3.0, 13.0) | - |
| Days between fix to final follow up - Mean (SD) | 53.9 (18.3) | 61.3 (29.4) | - |
| Median (IQR) | 50.0 (43.0, 57.0) | 55.5 (50.0, 62.8) | 0.011c |
| Range | (29.0, 160.0) | (35.0, 220.0) | - |
aT-test, bChi-squared test, cWilcoxon rank sum test, dFisher’s exact test.
Radiographic assessment of sagittal angulation, sagittal translation, and coronal translation had moderate interrater reliability, whereas assessment of coronal angulation had poor reliability (Table 5).
Table 5. ICC Inter-rater Reliability Analysis for the Radiographic Measures
| Outcome measures | ICC (95% CI) |
|---|---|
| Sag Angulation | 0.73 (0.61,0.83) |
| Cor angulation | 0.61 (0.46,0.74) |
| Sag trans | 0.71 (0.57,0.82) |
| Cor trans | 0.67 (0.53,0.79) |
Discussion
While children tolerate greater fracture displacement than their adult counterparts, initial care of these fractures remains imperative in determining definitive management. Though many factors influence the clinical course of these injuries, we focused this effort to study one modifiable factor contributing to the ultimate outcome, primarily the choice of splint material and its ability to hold an adequate reduction with the goal of avoiding surgery.
Our study demonstrated no significant difference in rates of conversion to surgery or in final alignment when initially splinted with plaster versus fiberglass. This is consistent with prior research by Daines et al., which evaluated the moldability of plaster compared to fiberglass and soft cast material. While they reported improved molding precision with plaster compared to fiberglass in clubfoot, developmental dysplasia of the hip, and femur fractures, they found no difference in materials in the BBFF model.2 In contrast, the current study found that five of the six patients converted to surgery were initially splinted with fiberglass and this may represent a trend toward significance and requires further evaluation with larger cohorts of patients. Thus, with the current data available, when considering which material to use in an academic trauma setting, additional factors should be considered, including cost of material, ease of application, and parent/patient satisfaction with the construct.
At our institution, forearm fractures are initially immobilized in a sugartong splint. This technique has been validated in the literature as a successful construct for non-operative management.7,8 While many studies have attempted to demonstrate the validity of other constructs, results have been variable.3–4,6,11 In this study, the overall rate of conversion to surgery was 2.6%, reinforcing that regardless of splint material, sugartong splints maintain adequate reduction for clinical healing. This is a simple splint that can be widely implemented and used successfully as standard of care.
Previous literature on pediatric forearm fractures has reported a wide range of loss of reduction and conversion to surgery, anywhere from 5-75%.7,12,15–20 With 97% of our cohort healing without surgery, these results more closely resemble those by Wu et al. who reported a 91.3% success rate for non-operative management.14 Theories as to why our rates of surgery were lower than previously reported include having an in-house orthopaedic surgery resident and/or tolerance of greater fracture deformity at follow-up. It is possible that having an orthopaedic resident available for all forearm reductions may contribute to better initial reductions than historical data as opposed to reductions performed by non-orthopaedic trained providers.
Given the possibility of acceptance of residual deformity outside of widely accepted guidelines proposed by Noonan and Price, a secondary analysis was performed.1 Although these guidelines for operative intervention are accepted as standard of care, the clinical utility of their application is unclear. Our secondary analysis revealed that only 83% of our patients actually met acceptable alignment per these guidelines at their final follow-up. The patients who had presence of radiographic healing, lack of symptomatic pain, or decreased range of motion, and returned to normal daily activities without issue were not indicated for surgery by the treating attending physician regardless of their residual deformity. Further research is required to understand if accepting this increased deformity has any negative long-term impact for these patients. A follow-up study is currently underway to evaluate these patients to determine their long-term outcome after healing outside the current ranges for acceptable non-operative treatment.
There were other factors aside from splint material that predicted unacceptable final outcome.1 While in our multivariate analysis, older age did not increase the odds of an unacceptable BBFFx, patients who had unacceptable final fracture alignment were significantly older in our study. This echoes the results of Bowman et al. who found being older than 10 years old was predictive of failure of non-operative management of forearm fractures.12 Okoroafor et al. found significantly higher failure rates in overweight/obese children, and while our study did not definitively show BMI percentiles to be associated with unacceptable final alignment, higher raw BMI values were associated with less acceptable outcomes.13 Additionally, fractures presenting with greater initial and residual displacement after reduction (especially sagittal translation) were less likely to heal in acceptable alignment (Figure 2). While initial displacement is largely unmodifiable, understanding these trends may help providers counsel patients appropriately, understand the prognostic impact of these injuries, and consider re-reduction for residual displacement after reduction or surgical intervention.
This study should be viewed in light of its limitations. Our primary limitation being the study was designed to compare conversion to surgery between splint materials. At 2.6%, our conversion rate was much lower than historic rates reported in the literature. As a result, our study was underpowered for our original plan and despite there being a trend toward conversion to surgery with fiberglass, it is possible this difference remains underappreciated with our small patient population. However, our effect measures would support the conclusion that splint material does not contribute to reduction failure and subsequent surgery.
A second limitation is the randomization was imperfect. We attempted to randomize splint material but due to difficulty with material access and other logistical factors, there was inconsistent adherence by orthopaedic residents performing the procedures. This did not result in significant demographic differences between the two groups. There was also a brief pause in enrollment due to COVID-19 as research assistants were removed from the emergency department for safety reasons, which may have indeterminate effects on the data.
The reliability index for radiographic measurements were primarily moderate. While not ideal, this is likely consistent with reliability across the many providers who care for these injuries and reflects the challenge in measuring such small imperfections. We therefore opted to analyze translation as a percentile of the fracture width to capture this data more accurately and provide meaningful landmarks for providers assessing their own radiographs.
This study represents a contribution to the literature in evaluating non-operative treatment of distal radius and both bone forearm fractures in a sugartong splint, showing splint material to be an unlikely contributing factor to failure. However, it also highlighted a significant discrepancy utilizing the standardized ranges for acceptable final alignment and emphasized the difficulty with evaluating alignment in defining non-operative treatment success. Additional study is needed to comprehensively assess long-term outcomes of patients with asymptomatic residual deformity outside of previously accepted guidelines for non-operative treatment.
Disclaimer
No funding was received. The authors have no conflicts of interest to report related to the subject matter.
References
- Noonan KJ, Price CT. Forearm and distal radius fractures in children. J Am Acad Orthop Surg. 1998;6(3):146–156.
- Daines SB, Aronsson DD, Beynnon BD, et al. What is the best material for molding casts in children? J Pediatr Orthop. 2014;34(7):743-748.
- Webb GR, Galpin RD, Armstrong DG. Comparison of short and long arm plaster casts for displaced fractures in the distal third of the forearm in children. J Bone Joint Surg Am. 2006;88(1):9-17.
- Bohm ER, Bubbar V, Hing KY, et al. Above and below-the-elbow plaster casts for distal forearm fractures in children: a randomized controlled trial. J Bone Joint Surg Am. 2006;88(1):1-8.
- Paneru SR, Rijal R, Shrestha BP, et al. Randomized controlled trial comparing above- and below-elbow plaster casts for distal forearm fractures in children. J Child Orthop. 2010;4(3):233-237.
- Bong MR, Egol KA, Leibman M, et al. A comparison of immediate postreduction splinting constructs for controlling initial displacement of fractures of the distal radius: a prospective randomized study of long-arm versus short-arm splinting. J Hand Surg Am. 2006;31(5):766-770.
- Dittmer AJ, Molina D, Jacobs CA, et al. Pediatric forearm fractures are effectively immobilized with a sugar-tong splint following closed reduction. J Pediatr Orthop. 2019;39(4):E245-E247.
- Denes AE, Goding R, Tamborlane J, et al. Maintenance of reduction of pediatric distal radius fractures with a sugar-tong splint. Am J Orthop (Belle Mead NJ). 2007;36(2):68-70.
- Halanski MA, Halanski AD, Oza A, et al. Thermal injury with contemporary cast-application techniques and methods to circumvent morbidity. J Bone Joint Surg Am. 2007;89(11):2369-2377.
- McGraw KO, Wong SP. Forming inferences about some intraclass correlation coefficients. Psychol Methods. 1996;1:30-46.
- Neal KM, Osterbur TA, Kiebzak GM. Improving quality in the treatment of pediatric forearm fractures: minimizing the need for repeat intervention with long-arm extension casting. J Pediatr Orthop. 2020;40:329-333.
- Bowman EN, Mehlman CT, Lindsell CJ, et al. Nonoperative treatment of both-bone forearm shaft fractures in children: predictors of early radiographic failure. J Pediatr Orthop. 2011;31:23-32.
- Okoroafor UC, Cannada LK, McGinty JL. Obesity and failure of nonsurgical management of pediatric both-bone forearm fractures. J Hand Surg. 2017;42:711-716.
- Wu JC, Daley E, Koueiter DM, et al. Operating room intervention rates after orthopaedic resident-reduced pediatric both-bone forearm fractures. J Pediatr Orthop. 2020;40:228-234.
- Yang JJ, Chang JH, Lin KY, et al. Redisplacement of diaphyseal fractures of the forearm after closed reduction in children: a retrospective analysis. J Orthop Trauma. 2012;26:110-116.
- Monga P, Raghupathy A, Courtman NH. Factors affecting remanipulation in paediatric forearm fractures. J Pediatr Orthop. 2010;19:181-187.
- Voto SJ,Weiner DS, Leighley B. Redisplacement after closed reduction of forearm fractures in children. J Pediatr Orthop. 1990;10:79-84.
- Proctor MT, Moore DJ, Paterson JM. Redisplacement after manipulation of distal radial fractures in children. J Bone Joint Surg Br. 1993;75:453-454.
- Edmonds EW, Capelo RM, Stearns P, et al. Predicting initial treatment failure of fiberglass casts in pediatric distal radius fractures: utility of the second metacarpal-radius angle. J Child Orthop. 2009;3:375-381.
- Hang JR, Hutchinson AF, Hau RC. Risk factors associated with loss of position after closed reduction of distal radial fractures in children. J Pediatr Orthop. 2011;31:501-506.