
Surgical/Technical Tips
Sacropelvic Fixation with S2-Alar-Iliac (S2AI) Screws Via CT-guided Navigation
1Department of Orthopedic Surgery, Mayo Clinic, Rochester, MN
Correspondence: A. Noelle Larson, MD, Department of Orthopedic Surgery, Mayo Clinic, 200 1st Street SW, Gonda 14-130, Rochester, MN 55905. E-mail: [email protected]
Received: October 29, 2022; Accepted: December 18, 2022; Published: February 1, 2023
Volume 5, Number 1, February 2023
Abstract
Sacropelvic fixation is frequently used for the correction of complex pediatric spine deformities. S2-alar-iliac (S2AI) screws are a powerful method to obtain iliac fixation. Advantages include a medialized starting point that requires less soft tissue dissection, no need for connectors to the rod, and reduced screw head prominence. Though the technique for S2AI placement under free-hand and fluoroscopic techniques has been described, there is limited description of computed tomography (CT)-guided technique for the placement of S2AI screws in pediatric patients undergoing surgery for complex spinal deformity. The goal of this paper is to describe the technique for placement of S2AI screws via CT-guided navigation and compare it to traditional fluoroscopy and free-hand techniques.
Key Concepts
- Sacral fixation is often needed in children with neuromuscular disorders as a result of pelvic obliquity.
- Sacro-alar-iliac fixation provides superior fixation and may help avoid complications such as failure of fixation and nonunion at the spine-pelvis junction.
- Surgical navigation has been used to place pedicle screws for fixation and can help achieve safe and stable fixation, especially when instrumenting complex spinal anatomy.
- Similarly, surgical navigation may facilitate efficient placement of large sacro-alar iliac screws and this manuscript demonstrates that methodology.
Introduction
Sacropelvic fixation is a commonly used surgical technique for the treatment of complex pediatric and adult spinal deformity.1–5 Sacropelvic fixation is indicated for complex scoliosis, high-grade spondylolisthesis, pelvic obliquity, sagittal plane deformity, and sacral fractures.6 Fixation involving the ilium was historically performed with the Galveston technique in which the ilium is incorporated into the construct by inserting rods between the inner and outer cortices of the ilium7; however, with the evolution of pedicle screw instrumentation, the use of iliac screws was adopted in the early 2000s.8,9 While the use of iliac screws has been a successful instrumentation technique, these screws have been associated with implant prominence, failure at the rod and screw connector, screw fracture, and pseudarthrosis.1,4,8,10
Sacropelvic fixation with the use of S2-alar-iliac (S2AI) screws has become the standard method for obtaining iliac fixation in both pediatric and adult patients.1–5,8,10–13 The purported advantages of these screws derive from the fact their starting point is 15 mm deeper and is more centralized than iliac screws.5,14 With a deeper and less lateral starting point, placement of these screws requires less dissection of the paraspinal musculature, eliminates the need for connectors, and minimizes implant prominence.5,14
S2AI screw placement, however, is not without complications. Adverse outcomes include injury to adjacent structures such as bladder, colon, or iliac vessels, cortical breaches, implant loosening, wound healing problems, infections, and pseudarthrosis.6 At 5-year follow-up, Abousamra et al. reported on rates of complications for pelvic fixation in cerebral palsy patients and found a lower rate of implant complications/pseudarthrosis with S2AI screws (0/19) compared to 11% (1/9) in unit rods, and 17% (7/42) with iliac screws.10
The trajectory and technique for S2AI screw placement in pediatric and adult patients was initially described by Chang et al.14 Since this report, various free-hand and image-guided techniques have been described.2–5,12,15 There are limited reports in the literature discussing the use of intraoperative computed tomography (CT)-based guidance for the placement of S2AI screws in pediatric patients. The purpose of this paper is to describe the technique for placement of S2AI screws via CT-guided navigation and compare results to traditional fluoroscopy and free-hand techniques.
CT-guided Surgical Technique
Patients are positioned prone on a Jackson radiolucent table and sterilely prepped and draped. The sacrum including the S2 foramen is exposed with care not to violate the thecal sac and to maintain good soft tissue planes. A reference frame (or fiberoptic calibration marker) is clamped to an exposed spinous process, and an intraoperative CT scan is obtained after the surgical field is covered by a sterile drape (O-arm, Medtronic, Inc., Louisville, CO). An optical camera records the position of the reference frame and CT scanner and automates registration of the images (Stealth, Medtronic, Inc., Louisville, CO). For a long fusion, the reference frame can be clamped to the spinous processes in the lower thoracic spine to achieve a clear trajectory. The reference frame can also be placed in the PSIS with care not to intersect the S2AI screw trajectory. Approximately, the S2AI screws and 2 to 3 vertebral levels can be incorporated in one scan, which includes the top of the acetabula and the sciatic notches up to the top of the sacrum. The scan should cover the patient’s pelvis to image the entire S2AI screw tract. The desired trajectory for S2AI screw placement is from the starting point, between the S1 and S2 lateral foramen along the lateral border, 10-20 mm superior to the sciatic notch aiming towards the anterior-inferior iliac spine (AIIS) (Figure 1).4,12,14 The screw will cross both cortices of the sacrum, traversing the SI joint, and the medial cortex of the ilium (Figure 1).
Figure 1. S2AI screw desired start point and trajectory. A) Starting point is between the S1 and S2 lateral foramen along the lateral border, 1-2 cm superior to the sciatic notch. B) The desired trajectory for S2AI screw placement is from the starting point towards the anterior-inferior iliac spine (AIIS). C) The screw will cross both cortices of the sacrum, traversing the SI joint, and the medial cortex of the ilium.

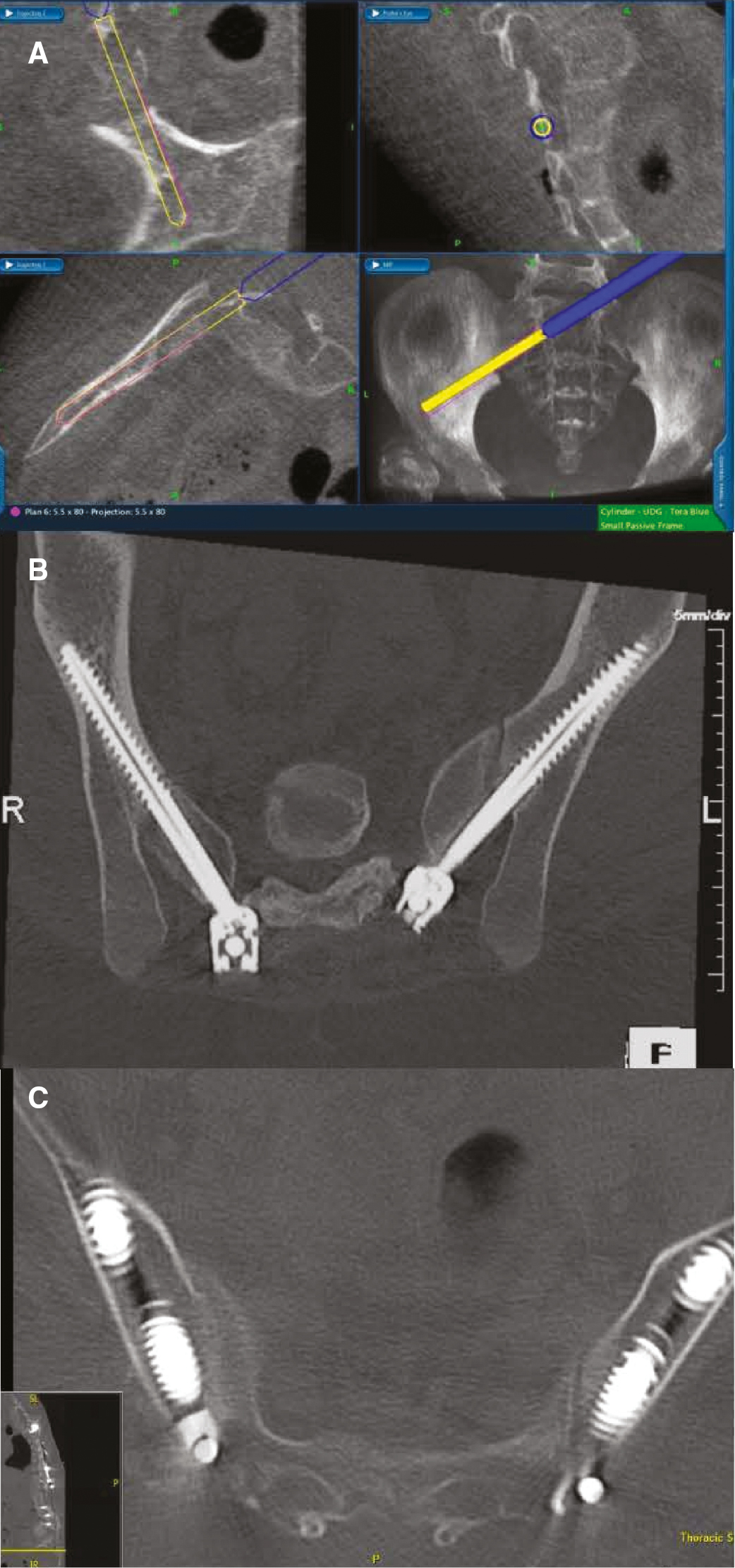
Using the data from the intraoperative or preoperative CT scan, a computerized navigation system is used for screw placement (Stealth, Medtronic, Inc, Louisville, CO; include 7D as well by SeaSpine). Referenced to the intraoperative CT data, the navigation system then generates real-time axial, coronal, and sagittal images depicting the position of the instrument or implant (Figure 2).
Figure 2. CT-guided technique for placement of S2AI screws. A) Computerized navigation system assists in screw placement, generating real-time coronal, axial, and sagittal images depicting the position of the instrument. B) & C) Postoperative axial CT images show optimal screw positioning.
Validity of the system is intermittently checked by placing a navigated probe on a known anatomic landmark and visually correlating the position to that shown on the image guidance system. This ensures that the reference frame had not shifted and that the guidance system is still producing correctly calibrated images. If there is any concern related to the accuracy of the intraoperative CT scan, an additional scan is obtained to verify the accuracy of the navigation or if a preoperative CT is used, the system can be re-registered.
Under image guidance with the navigated instruments, the S2AI screw tract is developed with a navigated straight awl or drilled with a navigated drill guide, and a cannulated wire is placed. Then the tract is probed and tapped and filled with the appropriate-sized screw. The guidewire should be withdrawn prior to screw placement so as to avoid breaking the guidewire. The width and depth of the screw tract are measured using the navigation system to allow screw diameter and length to be custom fit to the screw tract. Surgeons should aim to maximize screw length and diameter to optimize biomechanics of the fixation construct.1–3,13,16 As routine for spinal deformity cases, motor-evoked potentials and somatosensory potentials are monitored throughout the surgery.
Fluoroscopy Technique
Patient positioning and surgical approach for fluoroscopic placement of S2AI screws is similar, however, with traditional C-arm fluoroscopy draped into the sterile field. Figure 3 demonstrates operating room set up and technique for fluoroscopic technique. Once exposure has been obtained at the starting point, 2-4 mm lateral and 4-8 mm inferior to the S1 foramen, an en face view of the teardrop (formed by the medial iliac wall, lateral iliac wall, and sciatic notch inferiorly) is obtained to facilitate placement of the screw (Figure 3). The screw tract is developed with either a probe or a drill under fluoroscopic visualization. The trajectory is about 40 degrees lateral and 20-30 degrees caudal and 1-2 cm above the sciatic notch directed toward the AAIS, which can be guided using fluoroscopy. AP view of the pelvis helps to visualize position in relation to the sciatic notch, and the teardrop view ensures the pathway is in the thickest part of the ilium (Figure 3).6 Once the screw trajectory is created, the walls are probed, the tract tapped, and the appropriate-sized screw placed.
Figure 3. Fluoroscopic technique for placement of S2AI screws. A) & B) Operating room set up and patient positioning with traditional C-arm fluoroscopy draped into the sterile field. C) AP view of the pelvis helps to visualize position in relation to the sciatic notch. D) En face view of the teardrop is obtained to facilitate placement of the screw. E) Screw positioning can be confirmed again on AP view of the pelvis to verify placement.

Free-hand Technique
Free-hand technique for placement of S2AI screws has been previously described.4,12 The screws have the same entry point, just lateral to the midpoint between the S1 and S2 foramen. A burr is used to create a cortical breach at this point and a blunt pedicle probe is advanced toward the SI joint, directed toward the anterior inferior iliac spine by aiming cephalad to the posterior distal edge of the PSIS and perpendicular to the lateral sacral crest in order to avoid the sciatic notch inferiorly. Once the probe reaches the cortical surface of the SI joint, it is removed, and the tract is probed to check for cortical breeches. The pedicle probe is then reinserted and advanced through the SI joint and into the ilium toward the AIIS at a depth of about 70-90 mm. Once this trajectory is created, the walls are probed once more, the tract tapped, and the appropriate-sized screw placed.
Summary
CT Guidance in Pediatric Spine
The use of CT-guided navigation has been shown to successfully increase the accuracy of screw placement in pediatric spine surgery.15–18 Larson et al. found that the use of intraoperative CT and a 3D navigation system significantly improved the accuracy of pedicle screw placement in pediatric patients undergoing surgery for spinal deformity correction.18 CT-guided navigation was also shown to significantly increase the accuracy and safety of thoracic pedicle screws placed in patients undergoing posterior spinal fusion for the management of adolescent idiopathic scoliosis.17 CT-guided navigation has been shown to be effective for the placement of S2AI screws with the purported advantage of allowing for accurate and safe screw placement that optimized the screw trajectory and ensures adequate screw length.2,3 Further, recent work from our center showed no difference in operative time between pediatric cases with freehand/fluoroscopy compared to CT-guided navigation.17
Comparison to Free-Hand Technique
While the use of CT-guided navigation has proven successful for the placement of S2AI screws, there are several reports in the literature discussing free-hand techniques for the placement of S2AI screws.4,13 One of the benefits of free-hand techniques is that without the use of intraoperative fluoroscopic guidance, surgeons are able to minimize radiation exposure both to patients and surgeons.4 While these reports indicate that S2AI screws can be safely placed with free-hand techniques, these studies have only focused on an adult patient population and do not account for the difficult anatomy often seen specifically in neuromuscular pediatric patients with severe spinal deformity. Shillingford et al., in their description of a free-hand technique for S2AI screws in adult patients, state that their results cannot be generalized to patients with long standing congenital or pediatric neuromuscular deformities due the alterations seen in the osseous pelvic anatomy of these patients.4 Pediatric patients presenting with complex spinal deformities often have underlying diagnoses that involve distorted pelvic anatomy and are often associated with poor bone quality.1,19 Placement of S2AI screws has an inherently high risk due to the close proximity of important visceral and neurovascular structures to the screw’s trajectory. Pediatric patients with complex spinal deformity and neuromuscular conditions frequently have altered bony anatomy. Thus, we have found CT-guided navigation to be particularly useful in this patient population. Further, we have utilized a low-dose protocol for the intraoperative CT scanner (80 mSv, 20 mA, 80 mAs), which results in significantly less radiation exposure than the manufacturer’s recommended settings.20,21 With the low dose pediatric protocol, one CT scan in a 60 kg patient is equivalent to approximately 85 seconds of fluoroscopic image, 0.65 mSv, or a two view thoracic spine radiograph.21
Comparison to Fluoroscopic Technique
Review of our institution’s use of S2AI screws demonstrated that the use of CT-guided navigation compared to traditional C-arm fluoroscopy allowed for the placement of significantly larger and wider S2AI screws (Table 1).
Table 1. Review of S2AI Screws Placed Under CT-Guided Navigation Versus Traditional C-Arm Fluoroscopy at Our Institution
| CT-navigated Group (n=28) | Fluoroscopy Group (n=14) | p-value | |
|---|---|---|---|
| Average Screw Length (mm) | 81.4 (range, 60-100) | 72.7 (range, 57.5-90) | P=0.021 |
| Average Screw Diameter (mm) | 7.9 (range, 5-9.5) | 7.4 (range, 6.5-8) | P=0.034 |
| Operative Time (min) | 563 (range, 281-774) | 514 (range, 339-698) | P=0.18 |
| Mean # of Total Intraoperative CT Scans | 2.3 (range 1-4) | - | - |
In a series of S2AI screws used for pediatric deformity at 5-year follow-up, Jain et al. report that 11% of patients in their series had evidence of screw fracture, all with screw diameters less than 9 mm.1 Based on these results, they recommend using S2AI screws with the largest diameter possible to help protect against screw fracture.1 In a biomechanical analysis of lumbosacral fixation, McCord et al. defined the pivot point of the lumbosacral spine in the middle osteoligamentous complex at the L5-S1 junction. They found that the most stable lumbosacral constructs were those that extended lumbosacral fixation anterior to this pivot point the furthest.22 Thus, screws with longer length and greater diameter are thought to be less likely to fail. Nottmeier et al. recommend the use of CT-guided navigation when placing S2AI screws so as to place the largest and longest screw possible to optimize the biomechanics of sacropelvic fixation.2 Ray et al. also mention the biomechanical importance of placing the largest and longest S2AI screws possible.3 They note that one of the benefits of image guidance is that it allows the surgeon to optimize the screw’s trajectory to allow for engagement of the dense cortical bone of the ilium in order to maximize the screw’s pullout strength.3 Moreover, the 3D imaging provided by CT-guided navigation allows for optimization of the screw trajectory, providing the surgeon with the ability to optimize the biomechanics of the fixation construct.23
Summary of CT Navigation for Placement of S2AI Screws
Sacropelvic fixation via S2AI screws has been shown to be safe and effective in complex pediatric spine deformity and has advantages over other sacropelvic fixation techniques.1,5,10,13,14 Given limited reports discussing the use of intraoperative CT-guidance for the placement of S2AI screws in pediatric patients undergoing surgery for complex spinal deformity, the present paper describes the technique for placement of S2AI screws via CT-guided navigation while also summarizing traditional fluoroscopy and free-hand techniques. Benefits of CT navigation for S2AI screw placement include increased precision as well as longer and larger screws, ensuring a safer technique and creating a stronger fixation construct. CT guidance does, however, require advanced technology, which may be associated with a learning curve as well as increased radiation to the patient. At our institution, both CT-guidance and fluoroscopy are used to place S2AI screws. The authors conclude that S2AI screws can be safely placed via the above techniques, and surgeons have the choice of their preferred technique given appropriate experience and resources.
Additional Links
- Johns Hopkins Medicine: Pelvic Fixation with Sacral-Alar-Iliac Screws for Patients with Neuromuscular Scoliosis
- VuMedi: De-Novo Scoliosis – Part 4/9: S2 Alar-Iliac Screw Insertion
Disclaimer
No funding was received. A. Larson: Consultant in Orthopediatrics for Stryker, nView, Zimmer, Medtronic, and Globus, with all funds directed to the Department of Orthopedic Surgery at Mayo Clinic; T. Milbrandt: Consultant in Orthopediatrics for DePuy Synthes, Medtronic, and Zimmer, with all funds directed to the Department of Orthopedic Surgery at Mayo Clinic. Mayo Clinic has patent 10667845B2 issues with A. Larson and T. Milbrandt as inventors.
References
- Jain A, Kebaish KM, Sponseller PD. Sacral-alar-iliac fixation in pediatric deformity: radiographic outcomes and complications. Spine Deform. 2016;4(3):225-229.
- Nottmeier EW, Pirris SM, Balseiro S, Fenton D. Three-dimensional image-guided placement of S2 alar screws to adjunct or salvage lumbosacral fixation. Spine J. 2010;10(7):595-601.
- Ray WZ, Ravindra VM, Schmidt MH, Dailey AT. Stereotactic navigation with the O-arm for placement of S-2 alar iliac screws in pelvic lumbar fixation. J Neurosurg Spine. 2013;18(5):490-495.
- Shillingford JN, Laratta JL, Tan LA, et al. The free-hand technique for S2-alar-iliac screw placement: a safe and effective method for sacropelvic fixation in adult spinal deformity. J Bone Joint Surg Am. 2018;100(4):334-342.
- Sponseller PD, Zimmerman RM, Ko PS, et al. Low profile pelvic fixation with the sacral alar iliac technique in the pediatric population improves results at two-year minimum follow-up. Spine (Phila Pa 1976). 2010;35(20):1887-1892.
- Shah SA. Sacropelvic Fixation Techniques. Neuromuscular Scoliosis Technical Monograph: Intra-operative techniques for complex deformities in a diverse patient population. 2012:5-16.
- Allen BL, Jr., Ferguson RL. The Galveston technique of pelvic fixation with L-rod instrumentation of the spine. Spine (Phila Pa 1976). 1984;9(4):388-394.
- Elder BD, Ishida W, Lo SL, et al. Use of S2-alar-iliac screws associated with less complications than iliac screws in adult lumbosacropelvic fixation. Spine (Phila Pa 1976). 2017;42(3):E142-E149.
- Emami A, Deviren V, Berven S, Smith JA, Hu SS, Bradford DS. Outcome and complications of long fusions to the sacrum in adult spine deformity: luque-galveston, combined iliac and sacral screws, and sacral fixation. Spine (Phila Pa 1976). 2002;27(7):776-786.
- Abousamra O, Sullivan BT, Samdani AF, et al. Three methods of pelvic fixation for scoliosis in children with cerebral palsy: differences at 5-year follow-up. Spine (Phila Pa 1976). 2019;44(1):E19-E25.
- Mazur MD, Ravindra VM, Schmidt MH, et al. Unplanned reoperation after lumbopelvic fixation with S-2 alar-iliac screws or iliac bolts. J Neurosurg Spine. 2015;23(1):67-76.
- Park JH, Hyun SJ, Kim KJ, Jahng TA. Free hand insertion technique of S2 sacral alar-iliac screws for spino-pelvic fixation: technical note, acadaveric study. J Korean Neurosurg Soc. 2015;58(6):578-581.
- Jain A, Sullivan BT, Kuwabara A, Kebaish KM, Sponseller PD. Sacral-alar-iliac fixation in children with neuromuscular scoliosis: minimum 5-year follow-up. World Neurosurg. 2017;108:474-478.
- Chang TL, Sponseller PD, Kebaish KM, Fishman EK. Low profile pelvic fixation: anatomic parameters for sacral alar-iliac fixation versus traditional iliac fixation. Spine (Phila Pa 1976). 2009;34(5):436-440.
- Shabtai L, Andras LM, Portman M, et al. Sacral alar iliac (SAI) screws fail 75% less frequently than iliac screws in neuromuscular scoliosis. J Pediatr Orthop. 2017;37(8):e470-e475.
- McCord DH, Cunningham BW, Shono Y, Myers JJ, McAfee PC. Biomechanical analysis of lumbosacral fixation. Spine (Phila Pa 1976). 1992;17(8 Suppl):S235-S243.
- Baky FJ, Milbrandt T, Echternacht S, Stans AA, Shaughnessy WJ, Larson AN. Intraoperative computed tomography-guided navigation for pediatric spine patients reduced return to operating room for screw malposition compared with freehand/fluoroscopic techniques. Spine Deform. 2019;7(4):577-581.
- Larson AN, Santos ER, Polly DW, Jr., et al. Pediatric pedicle screw placement using intraoperative computed tomography and 3-dimensional image-guided navigation. Spine (Phila Pa 1976). 2012;37(3):E188-E194.
- Baaj AA, Beckman J, Smith DA. O-Arm-based image guidance in minimally invasive spine surgery: technical note. Clin Neurol Neurosurg. 2013;115(3):342-345.
- Barsa P, Frohlich R, Sercl M, Buchvald P, Suchomel P. The intraoperative portable CT scanner-based spinal navigation: a viable option for instrumentation in the region of cervico-thoracic junction. Eur Spine J. 2016;25(6):1643-1650.
- Ughwanogho E, Patel NM, Baldwin KD, Sampson NR, Flynn JM. Computed tomography-guided navigation of thoracic pedicle screws for adolescent idiopathic scoliosis results in more accurate placement and less screw removal. Spine (Phila Pa 1976). 2012;37(8):E473-E478.
- Maloney WJ, Rinsky LA, Gamble JG. Simultaneous correction of pelvic obliquity, frontal plane, and sagittal plane deformities in neuromuscular scoliosis using a unit rod with segmental sublaminar wires: a preliminary report. J Pediatr Orthop. 1990;10(6):742-749.
- Moshirfar A, Rand FF, Sponseller PD, et al. Pelvic fixation in spine surgery. Historical overview, indications, biomechanical relevance, and current techniques. J Bone Joint Surg Am. 2005;87(Suppl 2):89-106.