
Master’s Surgical Technique
Open Reduction and Pinning of Lateral Condyle Fractures
Shriners Medical Center Lexington, University of Kentucky, Lexington, KY
Correspondence: Vince Prusick, MD, Shriners Medical Center Lexington, 110 Conn Terrace, Lexington, KY 40508. E-mail: [email protected]
Received: December 16, 2022; Accepted: December 16, 2022; Published: February 1, 2023
Volume 5, Number 1, February 2023
Abstract
Lateral condyle fractures are the second most common elbow fracture in pediatric patients. Unlike supracondylar humerus fractures, these injuries involve the articular surface and present unique challenges. These injuries are graded based on the degree of displacement and this dictates your treatment. Both closed and open techniques are appropriate depending on the degree of displacement. Our preferred technique for open reduction and internal fixation is described and illustrated in the accompanying video.
Key Concepts
- Lateral condyle fractures are common elbow injuries in the pediatric population affecting the articular surface.
- Accurate reduction of articular surface is critical.
- In order to promote healing, these fractures often require longer immobilization than supracondylar fractures due to intraarticular nature of the injury.
- Blood supply to the capitellum enters posteriorly, so one must be cautious with posterior dissection.
Introduction
Lateral condyle fractures are the second most common elbow injury in pediatric patients.1 The injury involves a fracture line that propagates from the lateral distal humerus that extends down through the chondroepiphysis to the articular surface. Treatment is based on the degree of displacement and the ability to achieve an accurate and stable reduction of the articular surface. Unlike supracondylar humerus fractures, lateral condyle fractures are rarely associated with neurovascular injury; however, nonunion can occur due to the small area of bone in the fragment, and intraarticular nature of these injuries (synovial fluid) may prevent hematoma formation which is needed to begin the healing process. Failure to heal will lead to valgus elbow positioning and overgrowth of the lateral condyle and exuberant bone formation can lend to a varus appearance.
Most lateral condyle fractures result from a fall on the outstretched upper extremity and the varus force leads the extensor mechanism to pull the lateral condyle off to varying degrees. Minimally displaced fractures (2–4 mm) will hinge laterally and have an intact or minimally displaced articular surface that can prevent displacement and facilitate reduction with direct pressure (Figure 1).
Figure 1. The vast majority of lateral condyle fractures result from avulsion of the lateral condyle with the arm in varus. Minimally displaced fractures may have an intact or minimally displaced articular hinge that facilitates closed reduction (red bracket). While an archaic classification, this fracture represents a Milch 2 fracture.
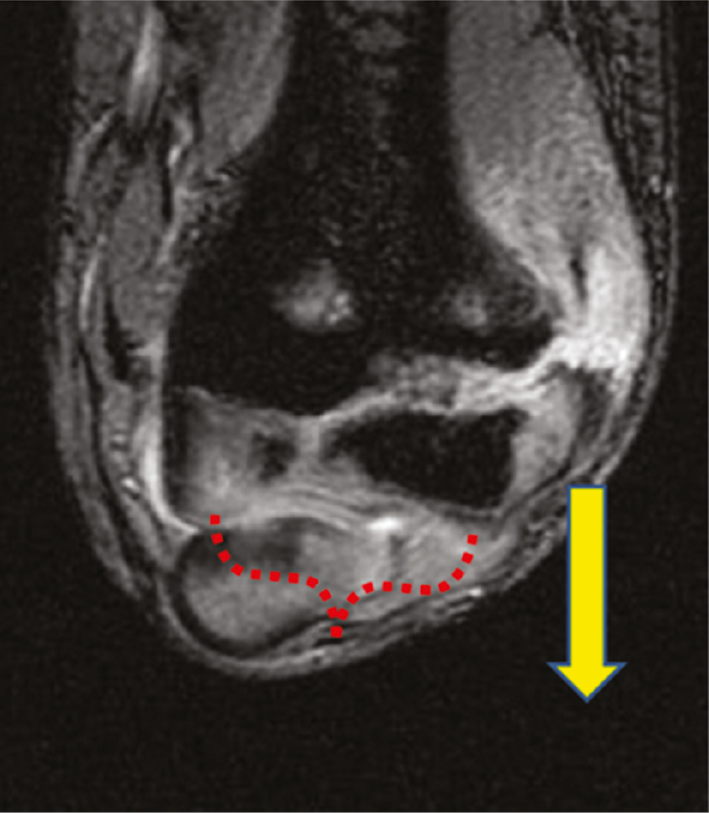
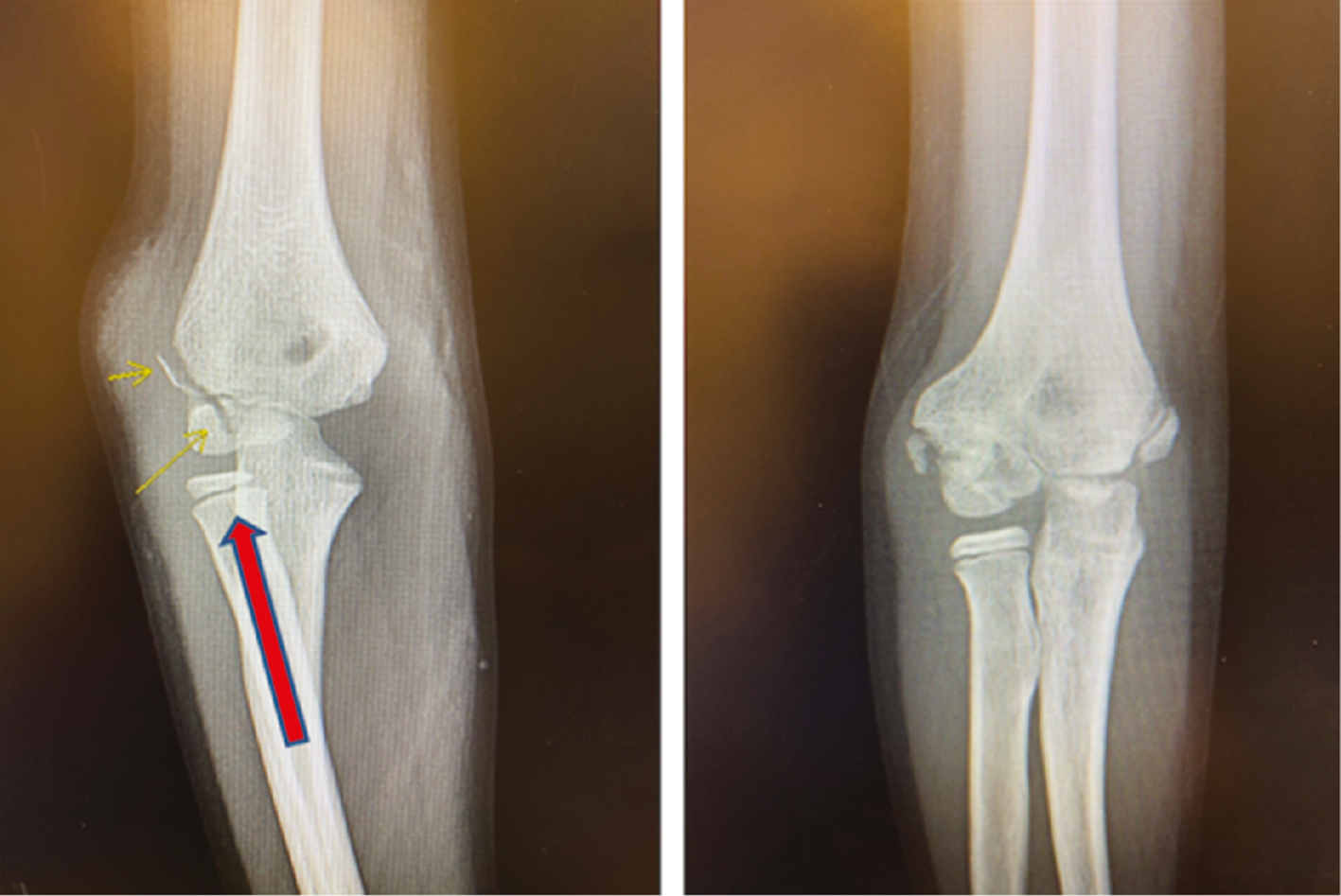
Rarely does a lateral condyle fracture result from an axial load in valgus that shears the lateral condyle proximally and always disrupts the articular surface (Figure 2). These are much harder to reduce closed and are more likely to require open reduction and internal fixation.
Figure 2. This intraarticular fracture (left) is likely a result of an axial load in valgus and can shear the lateral condyle off. Note the lateral elbow swelling. One year after closed treatment (right), the fracture has healed but is in slight cubitus varus. This would correspond to a Milch 1 fracture.
Description of the Method
Work-up and Diagnosis
A thorough history and physical examination along with complete radiographic work are essential for the evaluation of a child with a suspected lateral condyle fracture. While the exact mechanism (avulsion of the lateral condyle due to mobile wad pulling vs. direct impact of the proximal radius onto the lateral condyle) is debated, the child will typically present after a fall onto an outstretched hand. Swelling at the elbow, especially on the lateral side and often ecchymosis will be present. Movement at the elbow will likely be limited secondary to pain but the child typically remains neurovascularly intact distally.
Radiographs should include an AP, lateral, and internal rotation oblique of the distal humerus are recommended to evaluate the injury. Often the internal oblique will show the greatest degree of displacement which will ultimately guide treatment.2 Ordering an AP, lateral, and internal oblique x-ray of the elbow will not fully characterize the displacement, as these radiographs are not orthogonal to the distal humerus.
Decision-making
Jakob and Song have both described classification systems that can guide treatment.1,3 In minimally displaced fracture (<2 mm), closed treatment with a long arm cast and close observation is appropriate. For fractures with 2-4 mm of displacement, an attempt at closed reduction, percutaneous pinning, and arthrogram to assess articular congruity are recommended. Fractures with greater than 4 mm of displacement typically require open reduction and pinning, and articular alignment is assessed through direct visualization or via arthrogram. Additionally, an open fracture would be an indication for open reduction and pinning to allow for appropriate irrigation and debridement of the injury. Lastly, a nonunion would also require an open approach and internal fixation.
Treatment and Preoperative Planning
Once the decision to proceed to the operating room has been made based on the degree of displacement on quality radiographs, several pieces of equipment can be utilized to help with the procedure including sterile tourniquet, lighted suction or a head lamp, Kirschner wires (typically 2.0 mm), small Bennet or malleable retractors, and a reduction tool of choice (dental pick, point-to-point clamp, sterile fork, or surgeon’s thumb). Patient positioning is based on surgeon preference and can utilize either an arm table or the C-arm itself to support the elbow. It’s important that the surgeon positions a fluoroscopic monitor so that he or she can easily see it without turning around.
Operative Technique
OR set-up: The patient is positioned supine on the operative table and moved close to the edge of the bed. It can be helpful to secure the head with a towel and tape in a neutral position or use an anesthesia “Christmas tree” with donut foam to keep the head from falling off the bed. Depending on surgeon preference, the arm can be placed upon the hand table and fluoroscopy can be maneuvered in for an AP or lateral view. Alternatively, the C-arm is flipped so the image receiver can act as the table and is brought in from the foot of the bed so that the cranial and lateral aspect of the elbow are free of interference for the surgeon to stand (Figure 3). Fluoroscopy viewing screens should be positioned so that there is an unobstructed view when you are facing the elbow and will not need to turn away from the surgical field.
Figure 3. Suggested patient positioning using the C-arm as the operative surface. The surgeon can rotate the arm to get appropriate views.

Operative Technique: The patient is prepped and draped with an extremity drape to expose up to the shoulder. An attempt at a closed reduction can be performed utilizing elbow varus and forearm pronation to disengage the fragments followed by supination and elbow valgus.4 Direct pressure with the surgeon’s thumb can improve the reduction (Figures 4–7).
Figure 4. A minimally displaced lateral fracture is partially reduced with thumb pressure.

Figure 5. A single K-wire is used to provisionally fix lateral condyle fracture.

Figure 6. Further compression can be obtained by using a cannulated depth gauge over the K-wire.

Figure 7. A second wire is divergently placed to prevent displacement, and a third wire will be placed to finalize reduction.

If you are unable to achieve a successful closed reduction, a sterile tourniquet is then applied. A lateral/Kocher approach is used to access the fracture and complete the goals of surgery (Figure 8).
Figure 8. Lateral incision for fracture visualization. The incision is centered over the lateral condyle fragment (indicated by the circle on the image).

The incision is generous (5-7 cm) and curvilinear with the arm bent at 45 degrees, which forms a straight line with the arm in full extension. Sometimes it can be difficult to center, and with elbow swelling, it may be prudent to use fluoroscopy to draw out the incision. The deep dissection through the muscle has typically occurred from the injury and will direct the surgeon to the fracture and joint. Often the facia over the muscle is intact but hemorrhagic. Simple finger dissection through this area of hemorrhagic muscle will open this window up and allow easy exposure to the anterior aspect of the elbow joint (Figure 9).
Figure 9. For widely displaced fractures, the surgeon’s finger falls into the fracture site after the initial skin incision, and the elbow is irrigated to remove hematoma.

It is key to improve visualization by incising a small portion of the anterior capsule off the distal humeral fragment and extending the dissection distally until the radiocapitellar articulation is visualized. Dissecting off a small portion of the attached antero-lateral muscle from the lateral condyle fragment will complete the visualization needed to properly assess fracture reduction. Posterior dissection should be avoided to minimize risk to the capitellar blood supply (Figure 10).
Figure 10. Intraarticular inspection is facilitated by release of anterior capsule and muscle.

Small Bennet, Army-Navy, or malleable retractors can be placed carefully across the anterior aspect of the distal humerus to allow for inspection of the articular surface. It is important to thoroughly prepare the fracture bed in order for the fracture to reduce anatomically. A lighted suction tip or headlight can be very helpful to visualize the joint surface. A variety of instruments can be utilized for reduction including towel clip, dental pick, sterile fork, or the surgeon’s thumb. Reduction can be facilitated by relaxing the extensor muscles by keeping the wrist extended (Figure 11).
Figure 11. Keeping the wrist extended can help relax the extensor muscles and facilitate reduction.

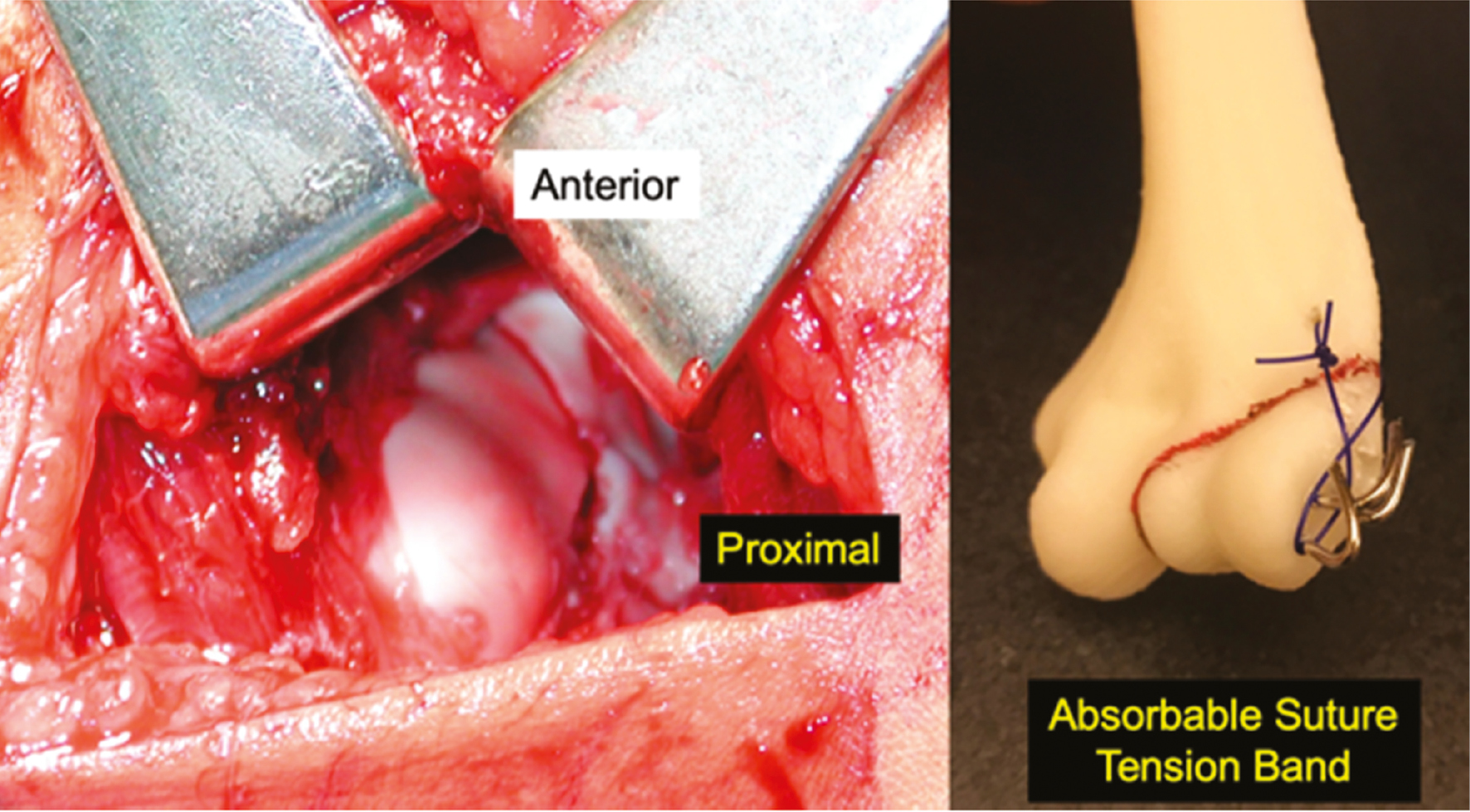
Occasionally, anatomic reduction of the articular surface will result in acceptable metaphyseal gapping. The surgeons’ focus should remain on reduction of the articular surface, and malreduction at the joint line can occur from the surgeon’s desire to anatomically reduce the metaphyseal component of the fracture (Figures 12 and 13).
Figure 12. Articular step-off is noted in this Milch Type 1 fracture.

Figure 13. The fracture is reduced at the articular surface and pinned. Use of an absorbable suture around the wires and through the metaphysis can reduce metaphyseal displacement.
Two or three K-wires are then inserted in a divergent fashion across the fracture site. Utilizing a two-pin construct, one pin should serve as the articular pin aiming for the medial epicondyle in a lateral to medial direction. The second pin should be directed up the lateral column with a goal divergence angle of at least 60 degrees if possible5 (Figure 14).
Figure 14. AP and lateral fluoroscopic images showing reduced and pinned lateral condyle fracture. Notice the ideal positioning of the two-pin configuration.

Success in this technically challenging procedure is best achieved with the use of an assistant—one surgeon holds reduction while another places the pins. Through direct visualization (Figure 15) and then palpation of the articular surface with a Freer elevator, the reduction is verified with fluoroscopic confirmation of reduction and proper pin placement. If there is concern about stability, a third pin can be placed in a divergent fashion. Good results have also been achieved utilizing a single 3.5/4.0 mm partially threaded, cannulated screw if greater stability is indicated. It should be oriented perpendicular to the fracture plane and often a second wire is placed to control rotation during drilling and screw insertion. This screw may become symptomatic in the future and necessitate elective removal.
Figure 15. Direct visualization of the articular surface of the distal humerus after closed reduction and pinning of the lateral condyle fracture. Notice the anatomic reduction of the articular surface (open arrow) with associated small amount of metaphyseal gapping superior to the articular surface (small arrow). Photo courtesy of Gregory Mencio, MD.

Postoperative Care
The patient is placed in a well-padded long arm cast or splint depending on personal preference. If a cast is utilized, it is recommended that bi-valving is performed to accommodate swelling. The patient is seen 1 week postoperatively to confirm maintenance of reduction and fixation and cast overwrap. Fixation will typically remain in place for 4 weeks at which time the cast is removed and radiographs are performed that confirm continued healing. Pins are removed at this time in the clinic setting and depending on the degree of healing, the child is either replaced back into a long arm cast for an additional 2 weeks or a removable posterior slab splint. Final follow-up occurs at 3 months with radiographs. If the patient has achieved radiographic union and normal range of motion, return to full activities is allowed and discharge from clinic is appropriate.
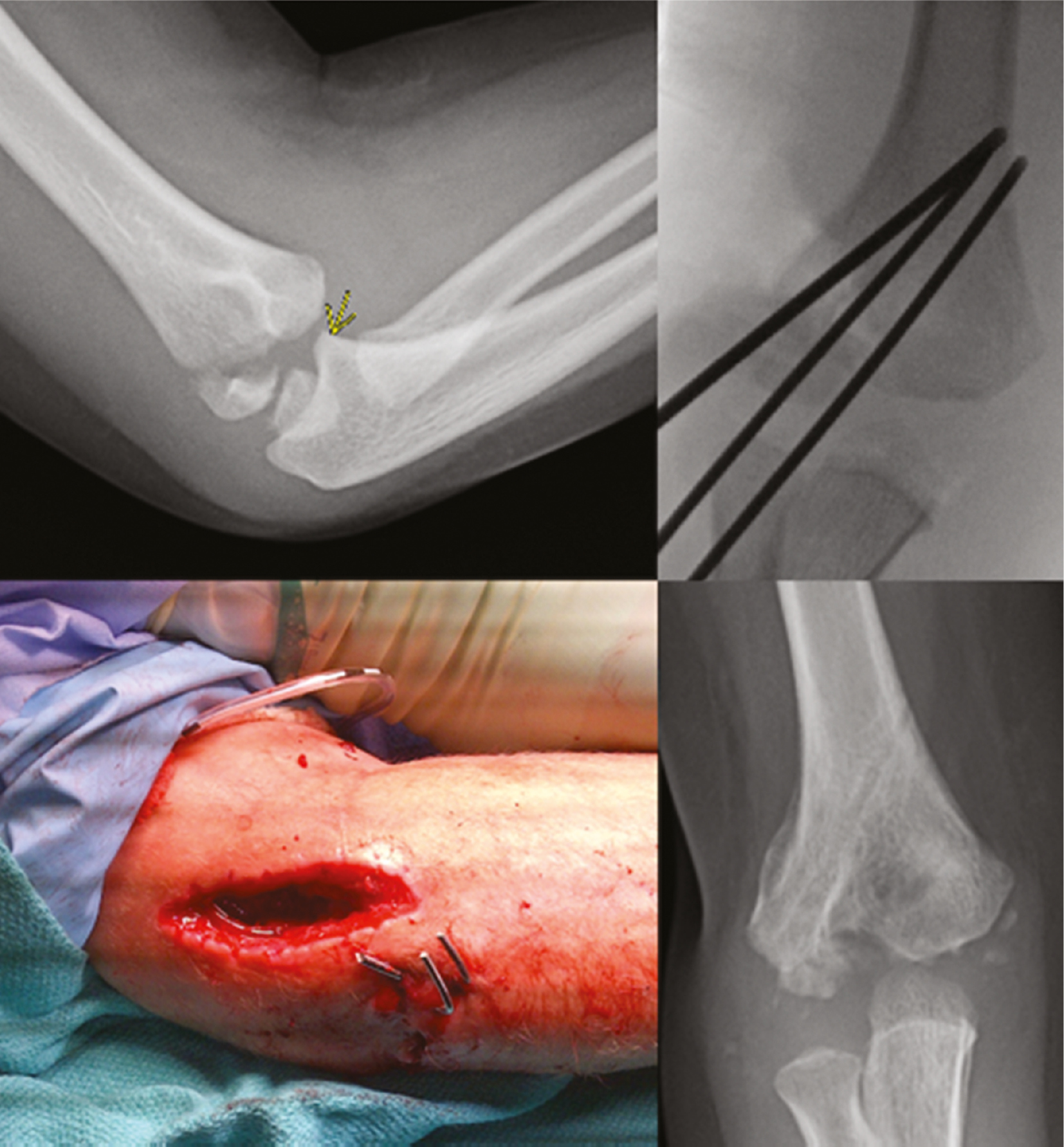
One complication that can occur from lateral condyle fracture pinning is septic arthritis developing from pin tract infection. It’s prudent to remember that pins used to stabilize these fractures are very commonly intraarticular; thus, pin tract inflammation/infection can lead to septic arthritis. For this reason, these pins are ideally removed within 4 weeks regardless of radiographic signs of healing (Figure 16).
Figure 16. This 5-year-old boy with a lateral condyle fracture developed septic arthritis and despite eventual healing, has signs of central humerus necrosis with an unknown natural history.
Summary
Lateral condyle fractures of the humerus are a common pediatric elbow injury. Treatment is dictated by the degree of displacement and can be achieved through both closed and open means. Anatomic restoration of the articular surface is paramount and the intraarticular nature of these injuries lends itself to several challenges not as commonly seen in supracondylar humerus fractures such as nonunion, avascular necrosis, infection, and lateral spurring.
Disclaimer
The authors have no conflicts of interest to report.
References
- Song S, Kang C, Min B, et al. Closed reduction and internal fixation of displaced unstable lateral condylar fracture of the humerus in children. JBJS. 2008;90:2673-2681.
- Song K, Kang C, Min B, et al. Internal oblique radiographs for diagnosis of nondisplaced or minimally displaced lateral condylar fracture of the humerus in children. JBJS. 2007;89A:58–63.
- Jakob R, Fowles J, Rang M, et al. Observations concerning fracture of the lateral humeral condyle in children. JBJS Br. 1975;57:430–436.
- Prusick V, Dantzker N, Hysong A, et al. Surgical technique for closed reduction and percutaneous pinning of pediatric lateral humeral condyle fractures. Tech Orthop. 2020;35:145-150.
- Bloom T, Chen L, Sabharwal S. Biomechanical analysis of lateral humeral condyle fracture pinning. J Pediatr Orthop. 2011;31:130-137.