
Current Concept Review
Posterior Column Osteotomies in Adolescent Idiopathic Scoliosis
1Department of Orthopedic Surgery, Vanderbilt University Medical Center, Nashville, TN; 2Department of Orthopaedic Surgery, Cedars-Sinai Medical Center, Los Angeles, CA; 3Department of Orthopedic Surgery, Akron Children’s Hospital, Akron, OH
Correspondence: Craig R. Louer Jr., MD, 2200 Children’s Way, Suite 4202, Nashville, TN 37212. E-mail: [email protected]
Received: December 19, 2022; Accepted: December 30, 2022; Published: February 1, 2023
Volume 5, Number 1, February 2023
Abstract
The posterior column osteotomy (PCO) is an adjunct technique for obtaining deformity correction during posterior spine fusion procedures. Full disarticulation of the posterior spinal column, including bony elements (namely the lamina and facet joints) and ligamentous complex is described as a PCO. This technique was originally described to allow for shortening of the posterior column during correction of excessive thoracic kyphosis; however, its indications have since been expanded to other spine deformities such as adolescent idiopathic scoliosis (AIS). Its expanded role in deformity surgery has been met with controversy: proponents tout increased flexibility and better spinal correction in three planes, while detractors cite lack of ostensible clinical benefit and potential for more complications. Differences in surgical technique are also prevalent. In this manuscript, we review the surgical technique of PCOs, including the traditional PCO as well as a modified posterior column release (PCR). Additionally, the controversy over when this technique should be utilized is further explored through summation of current literature on PCO outcomes.
Key Concepts
- The indications for posterior column osteotomies in pediatric spine deformity surgery are frequently debated, with the risk-benefit profile weighed differently among surgeons.
- Proponents of PCO use in scoliosis assert improved flexibility and correction of spinal deformity in three dimensions, in particular the ability to better restore thoracic kyphosis.
- Most studies acknowledge that there is an increased risk of a neuromonitoring alert when PCOs are performed, though a significant difference in postoperative deficits has not been described.
- The traditional Posterior Column Osteotomy PCO (i.e., “Ponte” osteotomy) is performed by creating a gap in the posterior elements which can be closed down with deformity correction (namely kyphosis).
- The modified Posterior Column Osteotomy (or Posterior Column Release [PCR]) can be performed by disarticulating the posterior tension band but leaving a smaller gap, perhaps limiting the ability for posterior compression but limiting spinal canal exposure.
Introduction
In 1945, Smith-Petersen originally described posterior column spinal osteotomies to correct kyphosis from ankylosed lumbar segments in rheumatoid arthritis. Complete facetectomy through both the superior and inferior articular facets corrected lumbar kyphotic deformity by transmitting leverage to the anterior column.1 In 1984, Alberto Ponte subsequently described a posterior column shortening osteotomy in the unfused thoracic spine to correct Scheuermann’s kyphosis. The “Ponte osteotomy” combines wide resection of the thoracic facet joints, laminae, and ligamentum flavum to generate 5-10 mm posterior gaps that close with compression through segmental instrumentation.2–5 Posterior column osteotomies (PCO) now are widely utilized for correction of hyper-kyphosis in the sagittal plane,5–9 as they allow an estimated 1 degree of kyphosis correction for every 1 mm of resection, resulting in up to 10 degrees of kyphosis correction per level.9,10
Indications for PCO have been expanded, including utilization with posterior spinal fusion (PSF) for correction of adolescent idiopathic scoliosis (AIS). The intended goal is to increase flexibility during three-dimensional deformity correction and restore normal sagittal plane parameters in the hypo-kyphotic thoracic spine by releasing the posterior tension band and lengthening the posterior column.11–15 However, the routine use of PCO for AIS remains controversial, with conflicting data as to the necessity, efficacy, and safety of this practice.16–18
Controversy
Surgeon approach to PCOs is highly variable in AIS. While some surgeons utilize PCOs routinely in every AIS case, others use them sparingly. National trends are increasing, with utilization recently doubling from 17% of AIS cases in 2007 to 35% in 2015.19 Proponents say that PCOs improve correction in all three planes of deformity. In an era of increased attention on the sagittal plane and a focus on correction of thoracic hypokyphosis in AIS, some surgeons thus routinely perform PCOs to increase posterior distraction and thoracic kyphosis. Detractors argue that PCOs increase the risk of neurologic injury and do not impart a meaningful benefit for routine AIS cases.
There is also controversy regarding surgical technique. Ponte originally described wide posterior resection for posterior column shortening, commonly performed with a Kerrison, while some surgeons have transitioned to a modified approach with an ultrasonic bone scalpel (UBS). There are also differences in the chronology of performing PCOs during AIS surgery (whether prior to or after pedicle cannulation and screw placement). In this paper, we aim to highlight anatomic considerations and technical pearls for performing PCOs.
Anatomy
Thorough understanding of the posterior column anatomy of the thoracolumbar spine is critical to the performance of PCOs.
Ligamentous structures requiring disruption:
|
Bony structures requiring disruption:
|
Technical Overview
Column Theory
The posterior spinal anatomy requiring resection for a PCO can be divided into medial and lateral structural elements (Figure 1). The posteromedial elements include the central lamina and the ligamentum flavum, while the posterolateral column is comprised of the superior and inferior articular facets. Temporally, the posteromedial and posterolateral columns may be addressed in varying order and at different points in the case to facilitate operative efficiency and safety. For instance, resection of the superior articular facets typically precedes pedicle screw insertion as screw heads may obstruct resection of the superior facet. However, the posteromedial column resection may be delayed until after pedicle screw insertion but immediately before rod insertion and deformity correction in order to reduce time that the spinal canal is exposed.
Figure 1. Medial and Lateral columns of the posterior spine can be resected at varying timepoints.

Traditional Posterior Column Osteotomy Technique
The traditional “Ponte-style” posterior column osteotomy for kyphosis dictates that symmetric gaps of 5-8 mm of the residual posterior elements are essential should be created in the posterior elements for uniform closure of the gaps with subsequent shortening of the posterior column. In severe or stiff deformities, Dr. Ponte advocated for wide resection from “pedicle to pedicle.”4
Modified Posterior Column Release Technique
In hypo-kyphotic deformities (fixed lordosis or AIS), a similar posterior column “release” (PCR) has been described.20 This technique acknowledges that inducing kyphosis requires relative lengthening of the posterior column. The same anatomic structures must be addressed, though reducing the size of the resection gap may be preferred, thereby minimizing exposure of the underlying neural elements to theoretically decrease risk of neurologic injury and/or pseudarthrosis. This has been advocated by some to be done with use of an ultrasonic bone scalpel (UBS) for the benefit of minimal bone resection, decreased blood loss,20 and theoretical improvements in efficiency and safety. The authors’ preferred methods for both the traditional and modified release osteotomy will be described for the thoracic spine.
Description of the Method
Common Preparation of Interspace for PCO (Figures 2 and 3)
- Wide subperiosteal exposure of the thoracolumbar spine is mandatory, including full visualization of the lateral aspect of each facet joint. Meticulous soft tissue dissection will pay dividends during the facetectomies and osteotomies
- Complete resection of the supraspinous and interspinous ligaments and removal of all soft tissue from posterior bony anatomy to facilitate eventual fusion
- Wide inferior facetectomies at all levels of intended fusion. This can be done in several ways including high speed burr, osteotomes, Capner gouge, and/or UBS. Remove remaining cartilage from the superior articular facet with burr or curette.
- Selection of levels for PCO based off pre-operative plan or intra-operative assessment
- Removal of spinous process and inferior lamina of the cephalad vertebra with a spinous process cutter and/or wide rongeur to expose the ligamentum flavum centrally, and the full extent of the superior articular facets laterally. Using a large rongeur, one can be rather aggressive about midline removal with little risk of inadvertent dural injury.
Figure 2. Sawbones representation of common level preparation for PCO. A) Every interspace in the operative field should have inferior facetectomies performed. B) Appearance following inferior facetectomy. C) Interspaces where PCOs will be performed will need spinous process and inferior lamina resection (colored in black), resulting in D) exposure of the superior articular facets (colored black) and ligamentum flavum (tan rectangle) for eventual resection and completion of PCO.
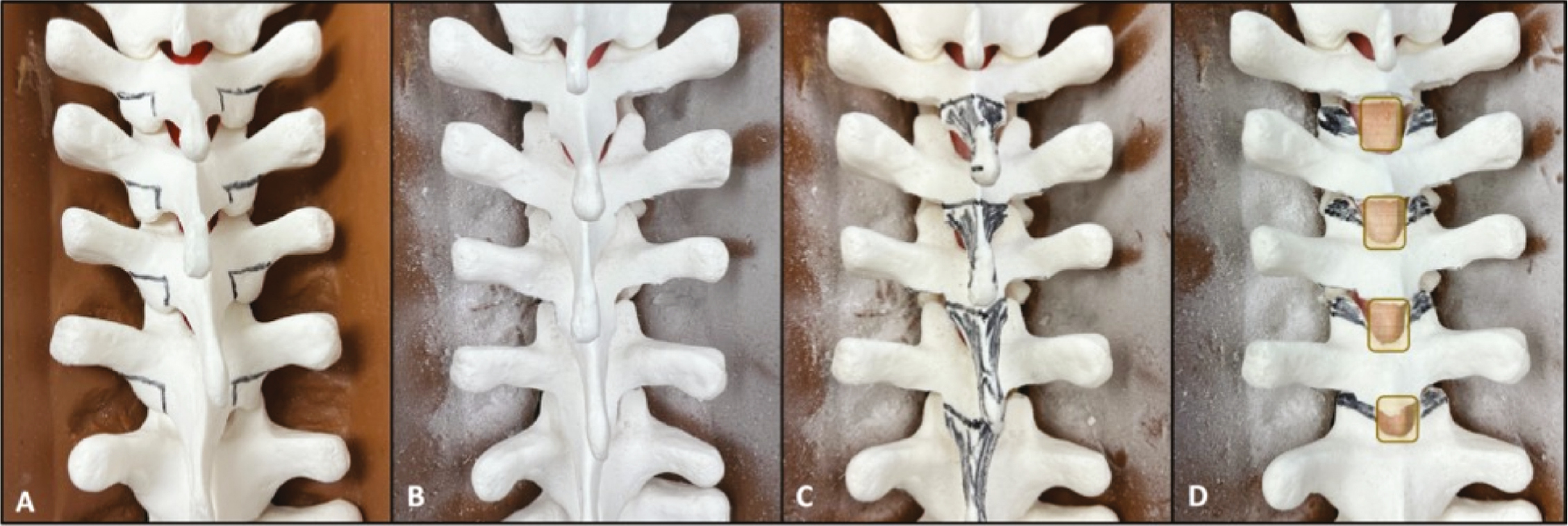
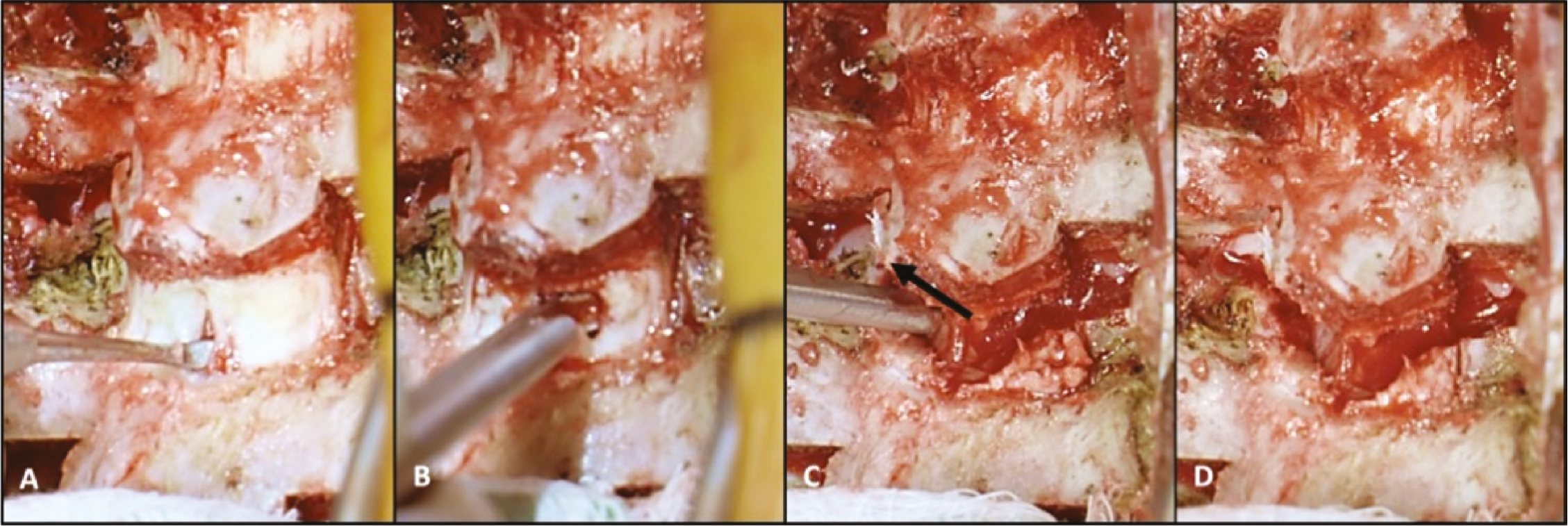
Figure 3. Surgical representation of common level preparation for PCO. A) Posterior spine following inferior facetectomies. B) Flexibility testing and deformity assessment to determine where PCOs may be beneficial. C) Removal of spinous process and inferior lamina at levels selected for PCO. D) Exposure of ligamentum flavum and superior articular facets following preparation steps.

Method for Traditional Posterior Column Osteotomy (PCO) (Figure 4)
- A large rongeur is used to remove the central portion of the ligamentum flavum. A midline rent in the ligamentum is visualized, often with outpouching of the epidural fat.
- A Woodson elevator is used to palpate the spinal canal through the midline rent on both the left and right side. With significant axial rotation, one can get an appreciation for the trajectory needed for the Kerrison rongeur (Figure 4A).
- A manual or pneumatic Kerrison rongeur21 is used to remove the ligamentum flavum (Figure 4B).
- The superior articular facet is removed bilaterally with the use of the Kerrison rongeur. The narrow osteotomy forms a “V” to resect the superior articular facet above the pedicle (Figure 4C).
- Gel foam with thrombin is used to cover the osteotomy site to aid in hemostasis and protect the exposed neural elements.
Figure 4. Method for Traditional Posterior Column Osteotomy (PCO). After thinning the ligamentum flavum (LF) with rongeur,
A) a Woodson elevator is used to palpate and dissect LF free from the epidural contents. B) Kerrison rongeur resects ligamentum flavum and C) superior articular facet bilaterally in a “V” shape. D) Completed PCO shows full disarticulation of the posterior spinal elements with symmetric gap for closure.
PCO Pearls and Pitfalls
- Use of a wide rongeur for resection of the posterior aspect of the ligamentum flavum can minimize inadvertent plunging into the canal.
- The inferior lamina can obstruct easy removal of the superior articular facet. Diligent removal of this prior to superior articular facet resection can reduce switching between instruments.
- In order to fully release the lateral facet capsule, one must ensure complete lateral resection. There is often a blood vessel adjacent to the facet that is torn with this last Kerrison release, which needs to be addressed.
- Curve location influences hazards encountered: the spinal cord is typically tight along the concavity while the epidural veins are typically present on the convex side where increased bleeding can be encountered.
- Once the spinal canal is exposed, all surgical assistants should be aware of the need for utmost care and diligence in preventing iatrogenic neural injury.
Method for Modified Posterior Column Release (PCR) (Figure 5)
Following exposure, inferior facetectomies, and spinous process/lamina excision:
- Cut the superior articular facet with UBS to complete posterolateral column resection (Figure 5A).
- We start lateral and work centrally to develop tactile feel for ventral cortex and avoid excessive canal or neuroforaminal violation.
- Avoid cutting into the pedicle. This will make release difficult and compromise your tactile feel of the UBS blade. Angle cut superolateral to inferomedial (“V” shaped like traditional method) and tilt hand towards the foot to improve safe-zone.
- When cut is complete, the superior aspect of the facet will often withdraw superiorly due to the release of tension. A controlled twist or push of the UBS blade can also confirm that there is mobility between the cut segments.
- Place hemostatic agent over cut facet. Proceed with segmental instrumentation.
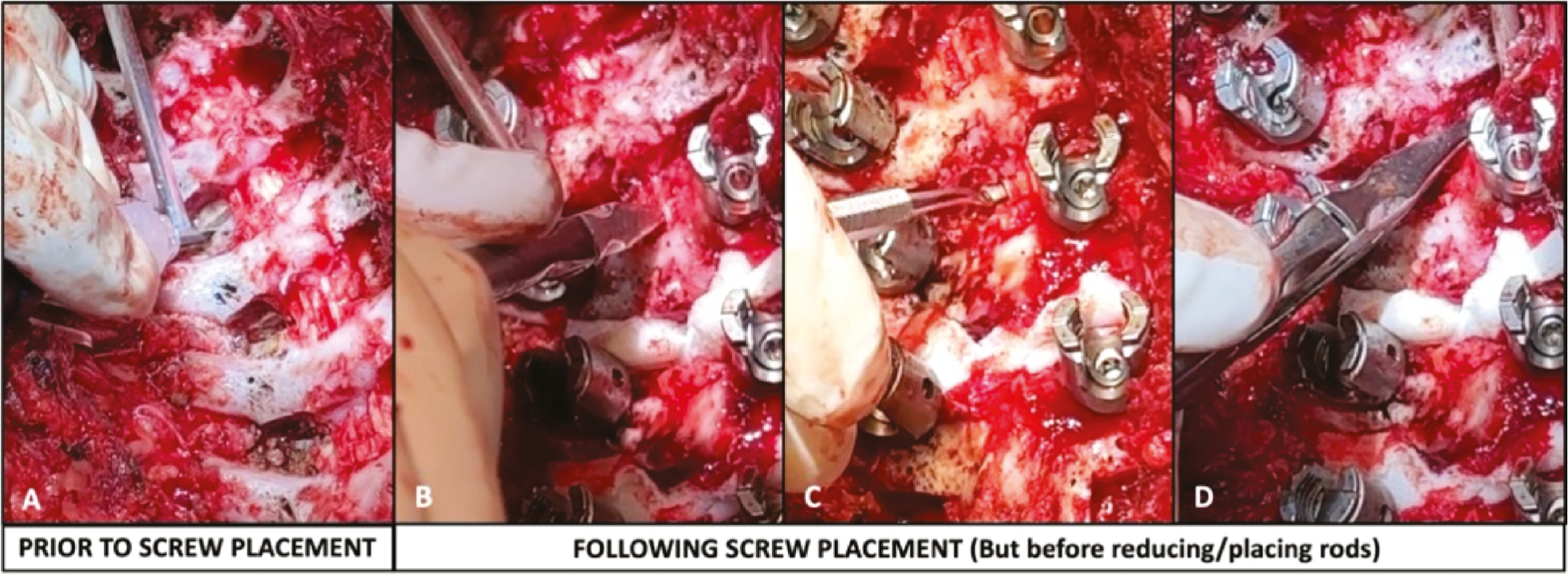
Figure 5. Method for Modified Posterior Column Release. A) Superior articular facets are cut with UBS prior to instrumentation. Following screw placement, the ligamentum flavum is resected starting with B) central resection with rongeur. C) Palpation/dissection with a Woodson elevator is performed prior to D) resection of ligamentum flavum with rongeur.
Following pedicle screw instrumentation but before rod insertion:
- Resection of ligamentum flavum to complete posteromedial column resection: use the same steps as above with rongeur, Woodson, and Kerrison (Figure 5B-D) to connect medial and lateral column and ensure tension band released.
- Place hemostatic agent and thrombin-soaked gel-foam over defect.
PCR Pearls and Pitfalls
- Interspaces with segmental lordosis may “spring open” when posterior tension band is fully disrupted. You may appreciate this to a lesser extent when the superior articular facet cut is completed, but the effect will be more pronounced when the ligamentum flavum resection is complete. This is a useful sign to demonstrate when your release is complete.
- FOR BOTH TECHNIQUES: Resect the most gravity-dependent levels and laterality first (typically most caudal and concave) then work “uphill.” If excessive bleeding is encountered, it will not disrupt visualization of subsequent resections.
- FOR BOTH TECHNIQUES: Consider placement of bone graft substitute “strips” (Figure 6) over the exposed neural elements to protect the dura and spinal cord from particulate bone graft, as there have been reports of bone graft impinging on the cord at the PCO site contributing to critical IONM alerts.18 Other alternatives include gel foam (See Video).
Figure 6. Placement of structural graft “strips.”

Outcomes of PCO
There have been highly variable reports of PCO outcomes. Many biomechanical studies demonstrate increased mobility from PCO with varying effects in each plane. Cadaveric studies comparing PCOs to specimens with intact facets found that PCOs reduce axial-plane derotational forces by 18%,22 while sequential PCOs improve flexion (+1.6°/osteotomy), extension (+1.5°/osteotomy), and axial rotation (+2.8°/osteotomy) with little effect on lateral bending motion.23 Likewise, Wang et al. concluded that PCOs increase flexibility in the axial and sagittal planes but have little effect on coronal correction, and overall gains are less effective than anterior releases.24 Interestingly, Holewijn et al. found 29.6% improvement in flexion and axial rotation after resection of the interspinous ligament, inferior facets, and ligamentum flavum, but sequential superior facetectomy provided no biomechanical benefit, thereby demonstrating the “law of diminishing returns.”17
Clinical results are even more variable, likely associated with difficulty isolating independent variables as many covariates may affect correction, including clinical factors such as gender, age, curve magnitude, and stiffness, and technical factors like rod material, rod size, implant type, implant density, deformity correction technique, and surgeon. The first large single-center cases series reporting the results of PCO to restore kyphosis in the hypokyphotic thoracic spine demonstrated increased T5-T12 kyphosis from 8 degrees to 18 degrees, and these AIS patients had 6% increased coronal correction with 8% IONM critical changes, but lacked a comparison group.14 Samdani et al. subsequently compared 125 Lenke 1 AIS patients with 4.3 ± 1.5 PCO to 66 unmatched controls and found that PCO improved the correction index from 62% to 67%, for a 3.3 degrees coronal plane improvement, 3.5 degrees kyphosis improvement, 15% rib prominence correction, though similar SRS scores.15
Other clinical studies have demonstrated little benefit from PCOs but potentially increased surgical risk. An unmatched comparison of AIS patients with and without PCO found no significant difference in coronal plane correction or kyphosis restoration while estimated blood loss (EBL) was 33 ml/level higher and operative time 8 min/level longer in the PCO group.16 In a single-center matched cohort of 68 patients, PCO provided no improvement in the sagittal or axial planes, only 8% improvement in coronal plane correction, and higher risk of critical neuromonitoring changes (15% with PCO vs. 0% without, p=0.05) with no difference in health-related quality of life (HRQoL).18
Other studies have likewise identified PCOs as an independent risk factor for intraoperative neuromonitoring (IONM) changes.25,26 Buckland et al. found that PCOs are an independent risk factor for IONM alerts (9.3% vs. 4.2%, p<0.001), though this did not manifest into a significantly different incidence of postoperative neurologic deficit (0.37% with PCO vs. 0.17% without, p=0.45).25 A large, unmatched, multicenter database study reported that patients with PCOs have higher risk of readmission and reoperation within 90 days but similar reoperation rate within 2 years while PCOs incur increased procedural cost resulting in a $15,854 higher mean hospital cost.19
Summary
Posterior Column Osteotomies (PCOs) for spine deformity surgery have controversial indications with debated outcomes. There are varying technical approaches for PCO performance, with traditional PCO and modified posterior column release (PCR) both having been described in the literature. Prospective randomized studies are needed on clinical outcomes for standard PCOs and the varying technical modifications.
Additional Links
- POSNAcademy: Traditional PCO in Scheuermann’s Kyphosis, Kira F. Skaggs, BA; Kenneth R. Kato, MS; Kenneth D. Illingworth, MD; Lindsay M. Andras, MD; David L. Skaggs, MD, MMM
- Operative Neurosurgery: Posterior Column Osteotomy
- POSNAcademy: Ponte Osteotomies, Paul Sponseller, MD
Disclaimer
C. Louer: Consultant – Depuy Synthes Spine; Research Support – NuVasive Spine – Shared support for research personnel, POSNA Zimmer Biomet Spine Research Grant; Royalties – Nsite Medical, Inc.; K. Illingworth: Consultant – Orthopediatrics; T. Metcalf: Position supported by NuVasive Spine educational grant; L. Flocarri: Nothing to disclose.
References
- Smith-Petersen MN, Larson CB, Aufranc OE. Osteotomy of the spine for correction of flexion deformity in rheumatoid arthritis. Clin Orthop Relat Res. 1969;66:6-9.
- Ponte A. Surgical treatment of Scheuermann’s hyperkyphosis. Orthop Trans. 1985;9:127.
- Ponte A. Posterior column shortening for Scheuermann’s kyphosis: an innovative one-stage technique. In: Haher TR, Merola AA, (eds). Surgical Techniques for the Spine. New York: Thieme; 2003:107-113.
- Ponte A, Orlando G, Siccardi GL. The true ponte osteotomy: by the one who developed it. Spine Deform. 2018;6(1):2-11.
- Geck MJ, Macagno A, Ponte A, et al. The Ponte procedure: posterior only treatment of Scheuermann’s kyphosis using segmental posterior shortening and pedicle screw instrumentation. J Spinal Disord Tech. 2007;20(8):586-593.
- McClendon J Jr, O’Shaughnessy BA, Sugrue PA, et al. Techniques for operative correction of proximal junctional kyphosis of the upper thoracic spine. Spine (Phila Pa 1976). 2012;37(4):292-303.
- Grevitt M, Kamath V, Avadhani A, et al. Correction of thoracic kyphosis with Ponte osteotomy. Eur Spine J. 2010;19(2):351-352.
- La Maida GA, Misaggi B. Posterior only treatment of adult thoracic kyphosis with multiple Ponte osteotomies and pedicle screw instrumentation. Eur Spine J. 2012;21(9):1891-1895.
- Cho KJ, Bridwell KH, Lenke LG, et al. Comparison of Smith-Petersen versus pedicle subtraction osteotomy for the correction of fixed sagittal imbalance. Spine (Phila Pa 1976). 2005;30(18):2030-2037; discussion 2038.
- Gill JB, Levin A, Burd T, et al. Corrective osteotomies in spine surgery. J Bone Joint Surg Am. 2008;90(11):2509-2520.
- Shufflebarger HL, Clark CE. Effect of wide posterior release on correction in adolescent idiopathic scoliosis. J Pediatr Orthop B. 1998;7(2):117-123.
- Shufflebarger HL, Geck MJ, Clark CE. The posterior approach for lumbar and thoracolumbar adolescent idiopathic scoliosis: posterior shortening and pedicle screws. Spine (Phila Pa 1976). 2004;29(3):269-276; discussion 276.
- Pizones J, Izquierdo E, Sanchez-Mariscal F, et al. Does wide posterior multiple level release improve the correction of adolescent idiopathic scoliosis curves? J Spinal Disord Tech. 2010;23(7):e24-30.
- Shah SA, Dhawale AA, Oda JE, et al. Ponte osteotomies with pedicle screw instrumentation in the treatment of adolescent idiopathic scoliosis. Spine Deform. 2013;1(3):196-204.
- Samdani AF, Bennett JT, Singla AR, et al. Do ponte osteotomies enhance correction in adolescent idiopathic scoliosis? An analysis of 191 Lenke 1A and 1B curves. Spine Deform. 2015;3(5):483-488.
- Halanski MA, Cassidy JA. Do multilevel Ponte osteotomies in thoracic idiopathic scoliosis surgery improve curve correction and restore thoracic kyphosis? J Spinal Disord Tech. 2013;26(5):252-255.
- Holewijn RM, Schlosser TP, Bisschop A, et al. How does spinal release and Ponte osteotomy improve spinal flexibility? The law of diminishing returns. Spine Deform. 2015;3(5):489-495.
- Floccari LV, Poppino K, Greenhill DA, et al. Ponte osteotomies in a matched series of large AIS curves increase surgical risk without improving outcomes. Spine Deform. 2021;9(5):1411-1418.
- Shaheen M, Koltsov JCB, Cohen SA, et al. Complication risks and costs associated with Ponte osteotomies in surgical treatment of adolescent idiopathic scoliosis: insights from a national database. Spine Deform. 2022;10(6):1339-1348.
- Bartley CE, Bastrom TP, Newton PO. Blood loss reduction during surgical correction of adolescent idiopathic scoliosis utilizing an ultrasonic bone scalpel. Spine Deform. 2014;2(4):285-290.
- Obana K, Kato K, Illingworth K, et al. Pneumatic powered kerrison rongeur in spine surgery can benefit patient and surgeon: surgical tips. J Pediatr Orthop Soc North Am. 2021;3(1). DOI: https://doi.org/10.55275/JPOSNA-2021-230.
- Wiemann J, Durrani S, Bosch P. The effect of posterior spinal releases on axial correction torque: a cadaver study. J Child Orthop. 2011;5(2):109-113.
- Sangiorgio SN, Borkowski SL, Bowen RE, et al. Quantification of increase in three-dimensional spine flexibility following sequential Ponte osteotomies in a cadaveric model. Spine Deform. 2013;1(3):171-178.
- Wang C, Bell K, McClincy M, et al. Biomechanical comparison of ponte osteotomy and discectomy. Spine (Phila Pa 1976). 2015;40(3):E141-E145.
- Buckland AJ, Moon JY, Betz RR, et al. Ponte osteotomies increase the risk of neuromonitoring alerts in adolescent idiopathic scoliosis correction surgery. Spine (Phila Pa 1976). 2019;44(3):E175-E180.
- Harfouch EB, Bunyan RF, Faraidy MA, et al. Ponte osteotomies increase risk of intraoperative neuromonitoring alerts in adolescent idiopathic scoliosis surgery. Surg Neurol Int. 2022;13:154.