
Tutorial on the Treatment of the Upper Extremity Dysfunction in Hemiplegia
Tutorial on the Treatment of the Upper Extremity in Cerebral Palsy: Patient Outcome
Harvard Medical School, Boston Children’s Hospital, Boston, MA
Correspondence: Carley Vuillermin, MBBS, MPH, FRACS, Boston Children’s Hospital, Orthopedic Center, 300 Longwood Ave., Boston, MA 02115. E-mail: [email protected]
Received: January 18, 2023; Accepted: January 23, 2023; Published: February 1, 2023
Volume 5, Number 1, February 2023
Treatment
Based on the patient’s functional goals, physical examination, and preoperative assessment, a decision was made to proceed with a SEMLS upper extremity hemiplegia reconstruction.
Procedures performed:
- ECU to ECRB transfer with Fractional lengthening of the FCU and FCR and Palmaris longus tenotomy for wrist extension
- Pronator teres rerouting for forearm supination
- Thumb reconstruction for improved functional positioning, including first webspace deepening with 4 flap Z-plasty, thenar muscle release, EPL rerouting through the first dorsal compartment, and thumb MCP sesamoidesis
Postoperative Immobilization and Occupational Therapy
The patient was immobilized for a total of 12 weeks postoperatively, and this course was split into 4-week intervals. For the first 4 weeks, the patient remained in a long arm cast in supination. For the second 4-week interval, she was transitioned into a long arm thermoplastic splint which was to be worn at all times except while at occupational therapy. Eight weeks postoperatively, the patient was transitioned to a below elbow thermoplastic splint to be worn during the day for 4 more weeks, wearing the above elbow splint at night. Nighttime splinting continued for 12 months postoperatively.
Spontaneous Functional Analysis: The patient has increased her SFA from a poor/active assist to predominantly active assist. There has been a modest improvement in her modified House functional level (Figure 1).
Figure 1. Comprehensive SHUEE examination score sheet.
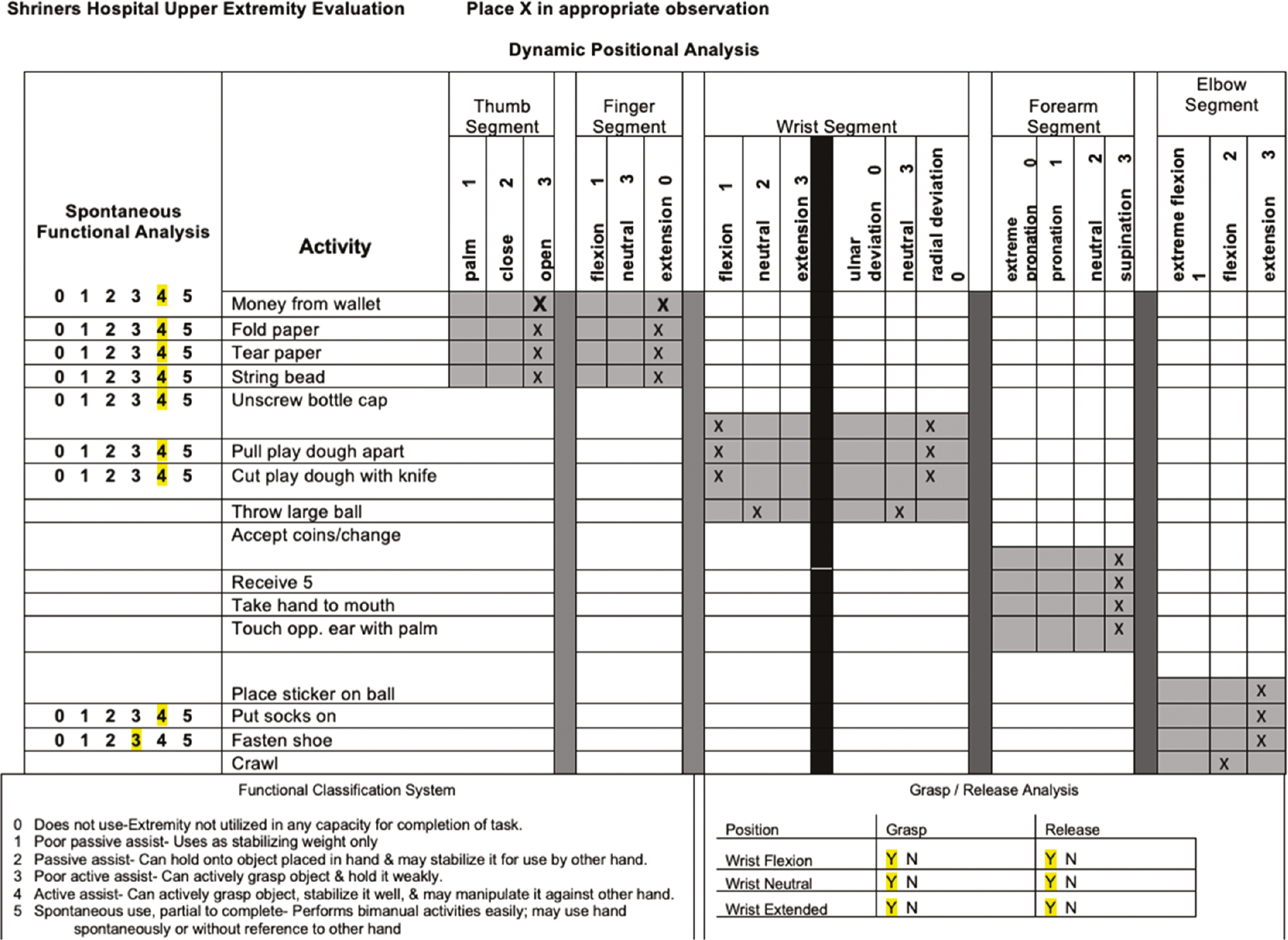
Dynamic Postural Analysis: The thumb segment remains open; however, there has been marked improvement in the first web with resolution of the MCP hyperextension (Figure 2). Her fingers still function in extension. Wrist extension has improved, she now functions in mild wrist flexion and radial deviation (Figure 3). Forearm supination function has shown the greatest consistent measurable change (Figure 4). See also Postoperative Video 1 and Postoperative Video 2 for dynamic patient outcome.
Figure 2. A) Preoperative – Patient grasping objects with thumb metacarpal adduction contracture and MCP joint hyperextension. B) Postoperative – 1st webspace is now open and MCP joint functions in mild flexion.

Figure 3. A) Preoperative – Wrist in marked flexion and ulnar deviation. b) Postoperative – Wrist now functions in mild flexion or extension. Dynamic thumb-in-palm deformity when grasping small objects.
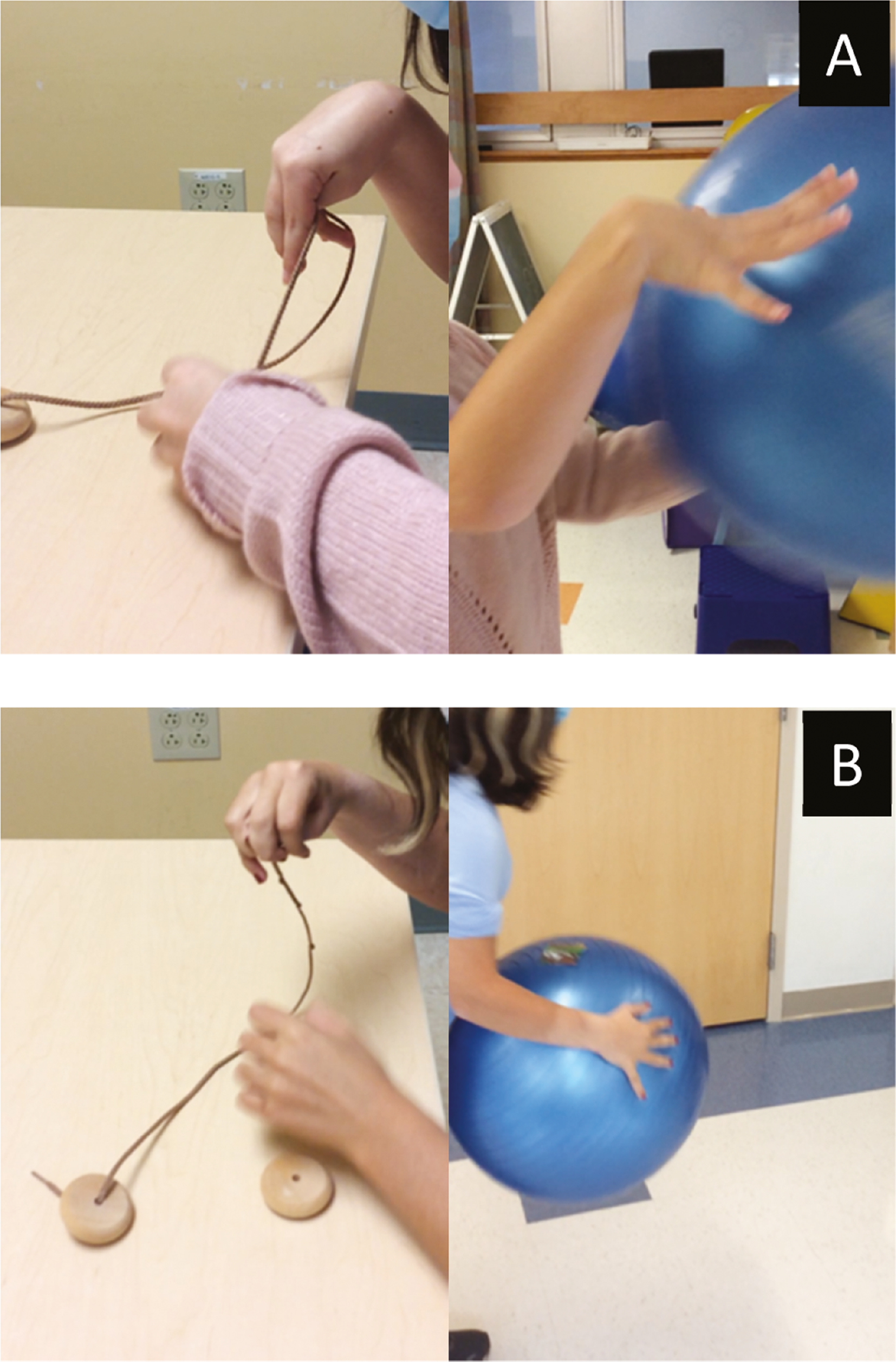
Figure 4. A) Preoperative – Forearm in neutral during activities requiring supination and unable to supinate to touch contralateral ear B) Postoperative – Able to actively supinate and bring palm to contralateral ear.

Grasp and Release Analysis: The patients grasp and release has been maintained in the postoperative situation. The thumb metacarpal is now out of the palm and therefore grasp and release is improved in wrist extension despite not having undergone finger flexor lengthening (Postoperative Video 3).
Summary
LA continues to have significant functional differences in her right upper extremity; however, she is very happy with the outcome and with appropriate preoperative goal setting, she is extremely pleased with her outcome. She continues to have some dynamic wrist flexion and thumb-in-palm deformity and will continue to need to work to maintain her new position. She may still require some selective tone management. Only long term will we see if the true balance is right for her. The decision to undertake a SEMLS reconstruction in patients with hemiplegia requires careful patient and operative selection by the surgeon in conjunction with the patient and their occupational therapist.
Disclaimer
The authors have no conflicts of interest to report.