
Original Research
Proximal Femoral Growth Alterations Can Be Seen Prior to Treatment of Developmental Dysplasia of the Hip: A Multicenter Cohort Study
1The Children’s Hospital of Philadelphia, Philadelphia, PA; 2BC Children’s Hospital, British Columbia, Vancouver, Canada; 3Arnold Palmer Hospital for Children, Orlando, FL
Correspondence: Wudbhav N. Sankar, MD, The Children’s Hospital of Philadelphia, Division of Orthopaedics, 3401 Civic Center Blvd., Philadelphia, PA 19104. E-mail: [email protected]
Received: February 13, 2023; Accepted: May 19, 2023; Published: August 1, 2023
Volume 5, Number 3, August 2023
Abstract
Background: Avascular necrosis (AVN), better considered proximal femoral growth disturbance (PFGD), following treatment for developmental dysplasia of the hip (DDH) remains poorly defined. In addition to limited reliability, it has been our experience that some radiographic features attributed to AVN/PFGD may be present prior to surgery. The purpose of this study was to determine the baseline prevalence of radiographic features suggestive of PFGD in a diverse cohort of patients with surgically treated DDH.
Methods: The prospectively collected database for an international multicenter study group was retrospectively queried for patients who underwent surgery for DDH with minimum 1-year radiographic and clinical follow-up. Preoperative radiographs were evaluated for findings typically used to define PFGD at follow-up. Development of actual AVN/PFGD was determined by consensus review of follow-up radiographs by three experts separate from this study. These experts (KM, CP, WS) were specifically selected by the study group to evaluate all patients in the database for development of AVN/PFGD. This occurred prior to the conception of this study.
Results: 145 patients were evaluated, with median preoperative age of 16.8 months (IQR:10.7-25.60). The proportion of patients with initial International Hip Dysplasia Institute (IHDI) grades of 2, 3, or 4 was 18%, 32%, and 50%, respectively. Prior to surgery, 20 hips (14%) had a heterogenous or “fragmented” epiphysis. Eight of the 145 epiphyses (6%) were significantly ellipsoid in shape. Depending on the definition, between 5-10% of hips had a wider neck at baseline compared to the contralateral, normal hip. At final follow-up, 42% of the hips were determined to have PFGD based on consensus review. Of all the patients that were considered to have PFGD at follow-up, 59% of patients had one feature of PFGD at baseline, and 20% had two or more.
Conclusions: The current study suggests that several factors used to define the development of PFGD following DDH surgery may be present prior to surgical intervention. Our data demonstrates that 20% of the patients who develop AVN have at least two markers of PFGD, per Salter criteria, prior to receiving any treatment. This suggests that some of these hips may not be morphologically “normal” at baseline and adds to the mounting body of evidence about the limitations of the Salter classification for AVN.
Level of Evidence: Level 2 – Prospective cohort study
Key Concepts
- Avascular necrosis classification systems in infantile DDH historically have had limited reliability and can be better thought of as proximal femoral growth disturbance (PFGD).
- Our study demonstrated that approximately 20% of the patients who were found to have postoperative PFGD/AVN actually had signs of proximal femoral growth disturbance prior to surgery.
- These findings suggests that some hips undergoing surgery for DDH may not be morphologically “normal” at baseline and add to the mounting body of evidence about the limitations of the Salter classification for AVN.
Introduction
Developmental dysplasia of the hip (DDH) is the most common congenital anomaly of the hip in children.1 Nonoperative treatments such as the Pavlik harness are largely successful when applied before 6 months of age. However, surgery is indicated for patients who present later in life or who fail nonoperative management. In spite of its general success, one of the most serious potential complications after bracing and surgical treatment for this condition is avascular necrosis (AVN) of the femoral head. This entity (which may be better termed proximal femoral growth disturbance [PFGD]) can lead to persistent acetabular dysplasia, degenerative osteoarthritis, and chronic hip pain.2 The Salter classification system has been historically used to define the presence or absence of AVN/PFGD in the first few years of life.3,4 However, recent studies have demonstrated that this classification system has only moderate interobserver reliability and prognostic value, demonstrating the need for a better objective classification system.5,6
In addition to these shortcomings of reliability, it has been our experience that some of the radiographic findings which are used to define PFGD, according to Salter’s criteria, may in fact be present prior to surgery. This suggests that some of these hips may not be morphologically “normal” at baseline and adds to the mounting body of evidence about the limitations of the Salter classification for AVN.7–10 The purpose of this study was to determine the baseline prevalence of radiographic features which are later deemed to be suggestive of PFGD in a multicenter patient population with surgically treated DDH.
Methods
The data for this study was queried from a prospective registry of a multicenter, international study group, the Global Hip Dysplasia Registry (GHDR), that collects data on infants and children treated for DDH. Institutional Review Board approval was obtained by all sites prior to patient enrollment. For each patient encounter, contributing surgeons collected and uploaded all relevant patient information and pertinent clinical details to a central database, including anteroposterior (AP) pelvic radiographs.
The deidentified database was queried between 2009 and 2021 to identify all patients who underwent operative intervention for DDH and had a minimum of 1-year radiographic follow-up. Patients were excluded for a missing baseline radiograph prior to treatment and less than 1 year of radiographic follow-up. As demonstrated in Figure 1, patients were excluded from analysis if there was an incorrect initial radiographic view, image artifact, or excessive rotation of the pelvis or femurs that prevented accurate assessment of acetabular and femoral morphology. Patients with bilateral dislocated hips were also excluded due to inability to compare to a healthy contralateral side.
Figure 1. STROBE inclusion figure.

Preoperative radiographs were analyzed as JPEGs downloaded from the overarching database and were evaluated using MicroDicom (General MicroDicom Ltd, 2021). This format precluded the ability to measure absolute distances in millimeters but did allow distance measurements in pixels that were compared to the normal contralateral side in order to calculate unitless ratios. All measurements were performed by two authors who were blinded to the ultimate outcome of each hip. The radiographic measurements included the ossific nucleus (epiphyseal) height and width, the physeal width, the narrowest width of the femoral neck, the length of the femoral neck, and the inter-trochanteric length (Figure 2). The length of the femoral neck was considered to be the perpendicular distance between the physis and the inter-trochanteric line (Figure 2, line 6). The density of the ossific nucleus/epiphysis was categorized as either homogenous or heterogeneous (Figure 3). To ensure reliability of each measurement, inter-rater reliability coefficients were calculated after 15% of the patients were reviewed by both independent reviewers (Table 1, Appendices 1 and 2).
Figure 2. Anteroposterior pelvic (AP) radiograph of an 18-month-old with IDHI grade 3 right-sided hip dysplasia. The figure demonstrates the acetabular and femoral measurements when evaluating for DDH and proximal femoral growth deformity. Hilgenreiner’s line (H) is a horizontal reference line between the triradiate cartilages. Perkin’s line (P) is a line perpendicular to Hilgenreiner’s line at the lateral corner of the acetabulum. Acetabular index (AI) is an angle created by a tangent to the bony acetabular roof and Hilgenreiner’s line. Lines 1-3 represent the ossific nucleus (epiphyseal) height, ossific nucleus (epiphyseal) width, and physeal width, respectively. Line 4 represents the narrowest femoral neck width, line 5 represents the inter-trochanteric line length, line 6 (dashed line between lines 3 and 5) represents the femoral neck length. Line 7 represents the subtrochanteric shaft width.

Figure 3. Anteroposterior radiograph of a 22-month-old male with right-sided DDH demonstrating broadening of the right femoral neck with eccentric and slightly fragmented femoral epiphysis.
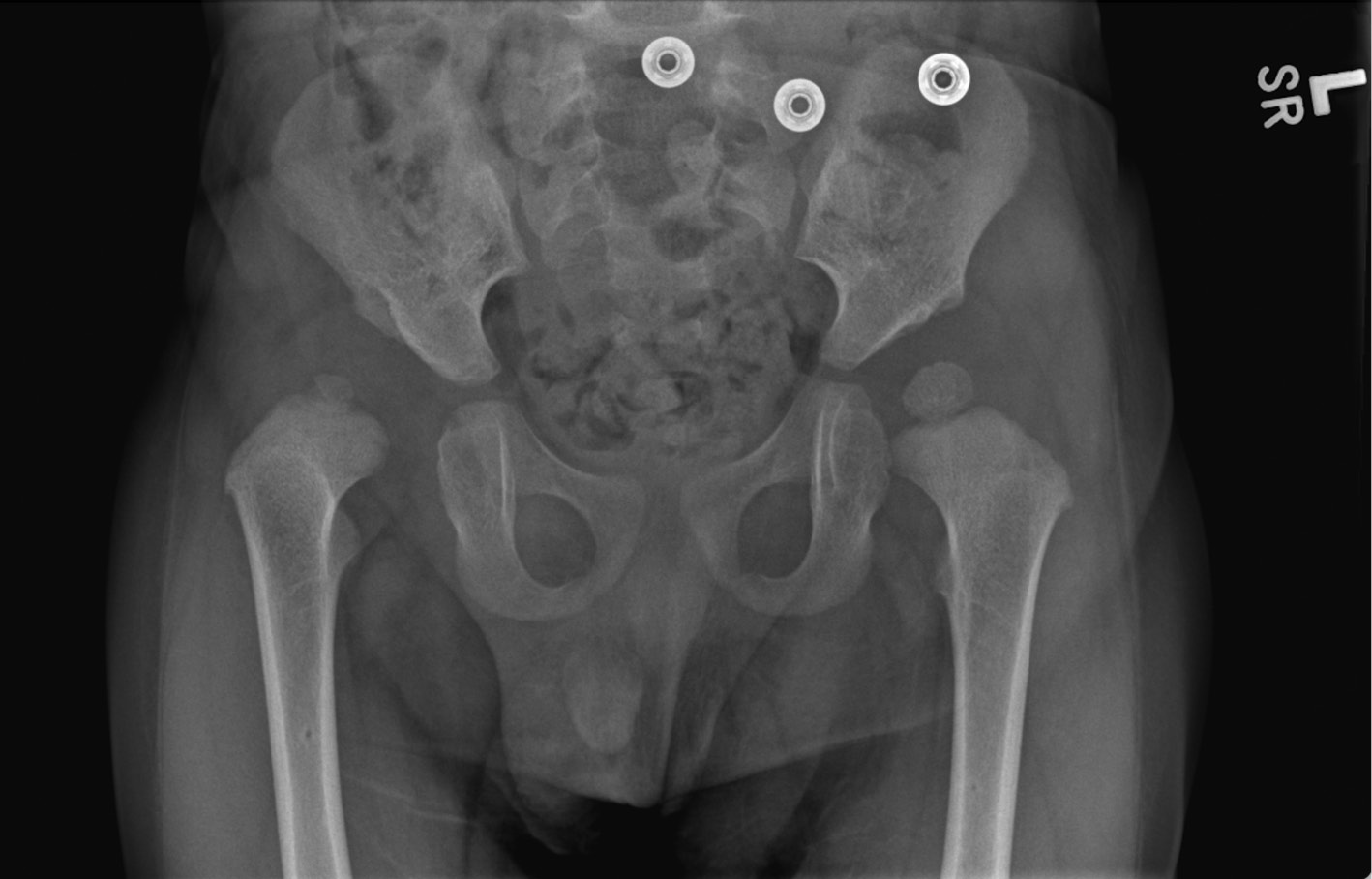
Table 1. Inter-Rater Reliability for All Hip Measurements
| Hip Measurements | Inter-Rater Reliability Coefficient | 95% Confidence Interval | P Value | Level of Agreement |
|---|---|---|---|---|
| Laterality of Hip Disease | 1a | - | 0.0001 | Perfect Agreement |
| Presence of Ossific Nucleus | 1a | - | 0.0001 | Perfect Agreement |
| Relative Size of Diseased to Healthy Ossific Nucleus | 0.754a | - | 0.0001 | Substantial Agreement |
| Shape of Ossific Nucleus (Symmetric vs. Eccentric) | 0.628a | - | 0.0001 | Substantial Agreement |
| Homogenous vs. Heterogenous Ossific Nucleus | 0.744a | - | 0.0001 | Substantial Agreement |
| IHDI Grade | 0.886a | - | 0.0001 | Near Perfect Agreement |
| Physeal Width | 0.986b | 0.975 to 0.992 | 0.0001 | Near Perfect Agreement |
| Femoral Neck Narrowest Width | 0.98b | 0.948 to 0.993 | 0.0001 | Near Perfect Agreement |
| Subtrochanteric Shaft Width | 0.989b | 0.98 to 0.994 | 0.0001 | Near Perfect Agreement |
| Femoral Neck Length | 0.988b | 0.979 to 0.993 | 0.0001 | Near Perfect Agreement |
| Inter-trochanteric Line Length | 0.979b | 0.96 to 0.989 | 0.0001 | Near Perfect Agreement |
| Ratio of Femoral Neck Length to Inter-Trochanteric line length | 0.931b | 0.881 to 0.96 | 0.0001 | Near Perfect Agreement |
| Epiphyseal Height | 0.974b | 0.944 to 0.986 | 0.0001 | Near Perfect Agreement |
| Epiphyseal Width | 0.981b | 0.96 to 0.99 | 0.0001 | Near Perfect Agreement |
| Ratio Epiphyseal Height: Width | 0.824b | 0.503 to 0.828 | 0.0001 | Near Perfect Agreement |
| Acetabular Index | 0.741b | 0.008 to 0.903 | 0.0001 | Substantial Agreement |
Inter-rater reliability calculated for categorical and continuous variables via a- Cohen’s Kappa Coefficient and b- Intraclass correlation (ICC) two-way mixed model with absolute agreement for single measures, respectively. Level of agreement: ≤0=Poor, .01–.20=Slight, .21–.40=fair, .41–.60=moderate, .61–.80=substantial, and.81–1=almost perfect.
The presence or absence of AVN/PFGD at most recent follow-up was determined by independent, blinded assessment of follow-up radiographs by three authors from three different institutions: The Children’s Hospital of Philadelphia, BC Children’s Hospital, and Arnold Palmer Hospital for Children; group consensus was reached for any discrepancies. Each reviewer based their designations on the Salter criteria (Table 2), but for the purposes of this manuscript, each hip was only classified with a simple “yes” versus “no.”3
Table 2. Salter Criteria for Avascular Necrosis of the Femoral Head
| Criteria | |
|---|---|
| 1 | Failure of the appearance of the ossifying nucleus of the femoral head for ≥ 1-year post-reduction |
| 2 | Failure of growth in an existing ossifying nucleus for ≥ 1-year post-reduction |
| 3 | Broadening of the femoral neck at 1-year post-reduction |
| 4 | Increased radiographic density of the femoral head followed by evidence of fragmentation |
| 5 | Residual deformity of the femoral head and neck at completion of re-ossification |
Statistical Analysis
Inter-rater reliability was calculated for categorical and continuous variables via Cohen’s Kappa coefficient and a two-way mixed model with absolute agreement for single measures, respectively. The ratio for each of the femoral head and neck measurements was calculated by comparing the diseased hip relative to the healthy hip for each patient. Neck width ratios greater than 1.05 and neck length ratios less than 0.95 were considered wide and short, respectively. Categorical variables are reported as frequency and percentage. Continuous variables are reported as mean and standard deviation or median and interquartile range for variables with non-normal distributions. The significance level was set at p-value <0.05. All statistical analyses were performed with SPSS software (IBM Corp, Armonk, NY).
Results
A total of 145 patients across 15 institutions were evaluated. Median age at the preoperative visit was 16.84 months (IQR: 10.65 to 25.60 mo.; Table 3). The proportion of patients with a pretreatment IHDI grade of 2, 3, or 4 was 18%, 32%, and 50%, respectively (Table 4). Ten patients (7%) had a history of previous orthosis treatment for a median of 61 days (IQR: 33 to 80 days; Table 3). Fifty-seven hips underwent closed reduction, 99 open reduction, and 67 open reduction with concomitant femoral and/or pelvic osteotomy. At final follow-up, 42% of the diseased hips (n=61/147) were determined to have some evidence of PFGD according to the three-surgeon panel.
Table 3. Overview of Patient Demographics and Disease Characteristics
| Variable | Total Population (n=145) |
|---|---|
| Sex | |
| Female | 123 (85%) |
| Male | 22 (15%) |
| Age at Imaging (months) | 16.84 (10.65 to 25.60) |
| Laterality of Disease | |
| Left | 97 (67%) |
| Right | 48 (33%) |
| Bracewear | |
| Pavlik Harness | 14 (10%) |
| Rigid Abduction Orthosis | 10 (7%) |
| Procedures | |
| Closed Reduction | 57 (39%) |
| Open Reduction | 99 (68%) |
| Osteotomy | 67 (46%) |
Data presented as n (%) or median (IQR).
Table 4. Overview of Hip Measurements in Total Patient Population
| Variable | Total Population (n=145) |
|---|---|
| Physeal Width Ratio | 0.86 ± 0.14 |
| Femoral Neck Narrowest Width Ratio | 0.89 ± 0.10 |
| Inter-trochanteric Length Ratio | 0.93 ± 0.08 |
| Femoral Length Ratio | 0.93 ± 0.14 |
| Ossific Nucleus Area Ratio | 0.50 ± 0.24 |
| Epiphyseal Height Ratio | 0.74 ± 0.17 |
| Epiphyseal Width Ratio | 0.64 ± 0.17 |
| Relative Size of ON (diseased: healthy) | |
| Absent | 26 (18%) |
| Smaller | 115 (79%) |
| Same Size | 1 (1%) |
| Larger | 3 (2%) |
| Ossific Nucleus Characterization | |
| Absent | 26 (18%) |
| Homogenous density | 99 (68%) |
| Heterogeneous density | 20 (14%) |
| Acetabular Index | 34 ± 5.9 |
| IHDI Grade | |
| 2 | 26 (18%) |
| 3 | 47 (32%) |
| 4 | 72 (50%) |
Reported ratios are diseased hip: healthy hip. Acetabular Index and IHDI grade are evaluating diseased hip only. Data presented as n ± SD, n (%).
*27 patients were missing ossific nucleus (ON) on the diseased hip, 7 of which were missing ON bilaterally.
At baseline, the ossific nucleus was present and smaller than the contralateral healthy hip in 79% (n=115/145) of patients and absent in 18% (n=26/145) of diseased hips. In hips missing the ossific nucleus, 50% (n=13/26) went on to develop PFGD, whereas, in patients with an ossific nucleus, 40% (n=48/119) went on to develop AVN (χ2=0.82, p =0.37). Considering the fourth Salter criteria for AVN/PFGD, 20 hips (14%) had a heterogenous or fragmented appearance of the epiphysis prior to surgery. An additional 8 patients (7%) had a markedly ellipsoid shape of the ossific nucleus preoperatively. At follow-up, 35% (n=7/20) and 88% (n=7/8) of these two groups were deemed to have PFGD (Table 5).
Table 5. Features of Preoperative Proximal Femoral Growth Disturbance Based on Salter Criteria
| Variable | Total Population (n=145) | Total Population of Patients who develop AVN (n=61) |
|---|---|---|
| Failure of Appearance and/or growth of ON | ||
| Missing ON | 26 (18%) | 13 (21%) |
| Smaller ON | 115 (80%) | 47 (77%) |
| Broadened Femoral Neck | ||
| Physeal Width Ratio > 1.05 | 15 (10%) | 4 (7%) |
| Femoral Neck Narrowest Width Ratio > 1.05 | 7 (5%) | 4 (7%) |
| Inter-trochanteric Length Ratio > 1.05 | 7 (5%) | 6 (10%) |
| Fragmentation of Femoral Head | ||
| Heterogenous Appearance of Femoral Epiphysis | 20 (14%) | 7 (11%) |
| Residual Deformity of Femoral Head and Neck | ||
| Short Femoral Neck Length | 91 (63%) | 42 (69%) |
| Total Population | 145 | 61 |
Data presented as n (%). The second column percentage is relative to the total population of those who develop AVN.
We evaluated neck morphology using three different metrics. On average, diseased hips had a slightly smaller physeal width, femoral neck width, and inter-trochanteric length compared to the contralateral side (Table 4). However, several patients had a broader neck according to physeal width ratio (15 hips, 10%), femoral neck width ratio (7 hips, 5%), and inter-trochanteric length ratio (7 hips, 5%). Four of 15 hips (27%), 4 of 7 hips (57%), and 6 of 7 hips (86%) in each group ultimately developed PFGD. Ninety-one hips in our series had a femoral neck length ratio less than 0.95 indicating some element of coxa breva at baseline. Forty-six percent (n=42/91) of these hips developed PFGD.
Of the patients that ultimately developed PFGD (n=61), 59% (n=36/61) of patients had one feature consistent with PFGD at baseline, 10% (n=6/61) had 2, and 10% (n=6/61) had 3 or more (Figure 4). The most common deformity was a short femoral neck length followed by an ellipsoid epiphysis and a heterogenous epiphysis (Table 5). There was no difference in the proportion of patients with baseline PFGD based on IHDI grade; however, there was a significant difference in the post-treatment PFGD based on IHDI grade (Tables 6 and 7).
Figure 4. Preoperative radiograph of a 24-month-old (A) shows left dislocated hip with slight widening and shortening of the left femoral neck (femoral neck width ratio 1.07). Postop radiograph (B) shows proximal femoral growth disturbance with coxa magna and widened/shortened femoral neck.

Table 6. Association of IHDI Grade with Baseline Proximal Femoral Growth Disturbance (1+ Marker)
| Variable | No Baseline PFGD | Baseline PFGD | Chi Square | P Value |
|---|---|---|---|---|
| IHDI Grade | 0.11 | 0.94 | ||
| 2 | 2 (7%) | 24 (93%) | ||
| 3 | 4 (9%) | 43 (91%) | ||
| 4 | 7 (10%) | 65 (90%) | ||
Preoperative proximal femoral growth disturbance includes at least one feature based on Salter criteria. IHDI grade are evaluating diseased hip only. Data presented as n (%). P value is significance level from Pearson Chi Square Test.
Table 7. Association of IHDI Grade with Development of Post-Treatment Proximal Femoral Growth Disturbance
| Variable | No Post-Op PFGD | Post-Op PFGD | Chi Square | P Value |
|---|---|---|---|---|
| IHDI Grade | 19.712 | 0.00005 | ||
| 2 | 22 (85%) | 4 (15%) | ||
| 3 | 33 (70%) | 14 (30%) | ||
| 4 | 29 (40%) | 43 (60%) | ||
IHDI grade are evaluating diseased hip only. Data presented as n (%). P value is significance level from Pearson Chi Square Test.
Discussion
The Salter criteria has historically been used to define AVN of the femoral head in patients treated for DDH.3 However, this classification scheme has recently been demonstrated to have only moderate inter-observer reliability, which limits its clinical utility.5,6 In addition, it has been our experience that some of the radiographic findings which have been used to define AVN may, in fact, be present prior to surgical intervention. It should also be noted that the term AVN itself, has started to fall out of favor. The Global Hip Dysplasia Registry (GHDR) has come to prefer the term proximal femoral growth disturbance to better describe these morphologic changes which may or may not be due to a vascular etiology.
Regardless, the purpose of this international multicenter study was to report the baseline prevalence of radiographic features consistent with PFGD in patients who have yet to undergo surgery for DDH. Preoperatively, 20 hips (17%) of those with an ossific nucleus already demonstrated a heterogenous or “fragmented” epiphysis. Eight of the 145 epiphyses (7%) were significantly ellipsoid in shape—another feature commonly attributed to PFGD. In terms of neck width and length (Salter criteria 3 & 5), we defined a broad neck as a transverse width 5% greater than the contralateral, unaffected side and a short neck as a length 5% shorter than the normal side. According to physeal width ratio (15 hips), femoral neck width ratio (7 hips) and inter-trochanteric distance ratio (7 hips), somewhere between 5-10% of all hips had broadened femoral necks at baseline. Ninety-one hips (63%) met our criteria for coxa breva prior to surgery. Out of our entire cohort, 36 of 145 hips (25%) had at least one baseline feature consistent with PFGD prior to surgical intervention, and 12 hips (8%) had at least two such features.
To our knowledge, this is the first study that evaluates the preoperative morphology of dislocated hips through the lens used to define postoperative PFGD.4,11–16 Our findings suggest that several of the features we currently use to define iatrogenic growth alterations may in fact be present at baseline. This further complicates our confidence in the Salter classification for postoperative AVN which has recently been shown to have only moderate interobserver reliability. The overall incidence of PFGD following surgical treatment for DDH has widely fluctuated in the literature, from 0-70%, secondary to the varying degrees of growth disturbance, different classification systems used to categorize such disturbances, and significant interobserver variability.4,11,17 Our current study suggests that differing baseline morphology of dislocated hips may be another source of variability in assessing postoperative PFGD.
This study utilized high-quality prospectively collected data; however, there remain several limitations. The degree of femoral rotation can vary between limbs and between patients. Although we attempted to control for rotation of the femurs through careful image selection and uniformly applied exclusion criteria, we could not control for minor deviations in femoral rotation which may affect our distance ratios. Another limitation, inherent in using a database with images saved in JPEG format, is that we were unable to measure actual distances on preoperative radiographs. Ratios of the diseased to healthy hip were calculated rather than using absolute measurements in order to account for differences in magnification and lack of normalization. This method of analysis also prevented the study from evaluating hips with bilateral disease, as there was not a healthy control hip with which to normalize measurements. Future single-center analysis and evaluation will be important to see if patients with bilateral disease have a similar prevalence of baseline proximal femoral growth disturbance. While this international database is one of the largest for the evaluation of DDH, we were still limited by small sample size for the description of patients with a baseline broadened femoral neck and development of AVN. This was due to a requisite of having a preoperative AP pelvis radiograph with a minimum of 1-year radiographic follow-up for all patients included in the study. Finally, it should be noted that the purpose of the present study was to draw attention to preoperative anatomic findings that may affect our assessment of postoperative PFGD; we did not intend to perform an exhaustive investigation into overall risk factors for AVN/PFGD. Such an investigation is separate and ongoing within our study group.
Regardless of its limitations, this multicenter study of infants undergoing operative treatment for DDH identified a significant prevalence of radiographic features consistent with PFGD in children prior to any surgical intervention. Moving forward, surgeons can utilize this information to improve awareness of preoperative anatomic findings that may later be considered postoperative AVN. Given the long-term morbidity of AVN, it is essential for surgeons to distinguish between baseline anatomic changes and pathologic treatment sequalae. Further studies are needed to better define proximal femoral growth disturbance and determine accurate risk factors for its development.
Disclaimer
The specific study group was funded by a registry grant from Pediatric Orthopaedic Society of North America. In addition, we want to acknowledge a fundraising partner, I’m a HIPpy Foundation. The authors report no conflicts of interest related to this manuscript.
References
- Shipman SA, Helfand M, Moyer VA, et al. Screening for developmental dysplasia of the hip: a systematic literature review for the US Preventive Services Task Force. Pediatrics. 2006;117:e557-e576.
- Malvitz TA, Weinstein SL. Closed reduction for congenital dysplasia of the hip. Functional and radiographic results after an average of thirty years. J Bone Joint Surg Am. 1994;76:1777-1792.
- Salter RB, Kostuik J, Dallas S. Avascular necrosis of the femoral head as a complication of treatment for congenital dislocation of the hip in young children: a clinical and experimental investigation. Can J Surg. 1969;12(1):44-61.
- Kalamchi A, MacEwen GD. Avascular necrosis following treatment of congenital dislocation of the hip. J Bone Joint Surg Am. 1980;62:876-888.
- Schaeffer EK, Ponton E, Sankar WN, et al. Interobserver and intraobserver reliability in the Salter classification of avascular necrosis of the femoral head in developmental dysplasia of the hip. J Pediatr Orthop. 2022;42(1):e59-e64.
- Tsukagoshi Y, Kamegaya M, Kamada H, et al. The correlation between Salter’s criteria for avascular necrosis of the femoral head and Kalamchi’s prognostic classification following the treatment of developmental dysplasia of the hip. Bone Joint J. 2017;99-B(8):1115-1120.
- O’Brien T, Millis MB, Griffin PP. The early identification and classification of growth disturbances of the proximal end of the femur. J Bone Joint Surg Am. 1986;68(7):970-980.
- Keret D, MacEwen GD. Growth disturbance of the proximal part of the femur after treatment for congenital dislocation of the hip. J Bone Joint Surg Am. 1991;73:410-423.
- Bradley CS, Perry DC, Wedge JH, et al. Avascular necrosis following closed reduction for treatment of developmental dysplasia of the hip: a systematic review. J Child Orthop. 2016;10:627-632.
- Novais EN, Hill MK, Carry PM, et al. Is age or surgical approach associated with osteonecrosis in patients with developmental dysplasia of the hip? A meta-analysis. Clin Orthop Relat Res. 2016;474:1166-1177.
- Weinstein SL, Dolan LA. Proximal femoral growth disturbance in developmental dysplasia of the hip: what do we know? J Child Orthop. 2018;12(4):331-341.
- Kim HW, Morcuende JA, Dolan LA, et al. Acetabular development in developmental dysplasia of the hip complicated by lateral growth disturbance of the capital femoral epiphysis. J Bone Joint Surg Am. 2000;82:1692-1700.
- Campbell P, Tarlow SD. Lateral tethering of the proximal femoral physis complicating the treatment of congenital hip dysplasia. J Pediatr Orthop. 1990;10:6-8.
- Gore DR. Iatrogenic avascular necrosis of the hip in young children: a long-term follow-up. J Pediatr Orthop. 1999;19:635-640.
- Herold HZ. Avascular necrosis of the femoral head in congenital dislocation of the hip. Isr J Med Sci. 1980;16:295-300.
- Herold HZ. Avascular necrosis of the femoral head in children under the age of three. Clin Orthop Relat Res. 1977;126:193-195.
- Bucholz R, Ogden J, eds. Patterns of ischemic necrosis of the proximal femur in nonoperative treated congenital hip disease. In: Sixth Open Scientific Meeting of the Hip Society. St. Louis, MO: C. V. Mosby; 1978.
Appendices
Appendix 1. Inter-Rater Reliability for Categorical Hip Measurements
| Overall Hip Kappa Correlations | Cohen’s Kappa | P Value | Level of Agreement |
|---|---|---|---|
| Laterality of Hip Disease | 1 | 0.0001 | Perfect Agreement |
| Presence of Ossific Nucleus | 1 | 0.0001 | Perfect Agreement |
| Relative Size of Diseased to Healthy Ossific Nucleus | 0.754 | 0.0001 | Substantial Agreement |
| Shape of Ossific Nucleus (Symmetric v. Eccentric) | 0.628 | 0.0001 | Substantial Agreement |
| Homogenous vs. Heterogenous Ossific Nucleus | 0.744 | 0.0001 | Substantial Agreement |
| IHDI Grade | 0.886 | 0.0001 | Near Perfect Agreement |
| Diseased Hip Kappa Correlations | |||
| Presence of Ossific Nucleus | 1 | 0.0001 | Perfect Agreement |
| Relative Size of Diseased to Healthy Ossific Nucleus | 0.684 | 0.0001 | Substantial Agreement |
| Shape of Ossific Nucleus (Symmetric v. Eccentric) | 0.567 | 0.0001 | Moderate Agreement |
| Homogenous vs. Heterogenous Ossific Nucleus | 0.698 | 0.0001 | Substantial Agreement |
| IHDI Grade | 0.785 | 0.0001 | Substantial Agreement |
| Healthy Hip Kappa Correlations | |||
| Presence of Ossific Nucleus | 1 | 0.0001 | Perfect Agreement |
| Relative Size of Diseased to Healthy Ossific Nucleus | 0.705 | 0.0001 | Substantial Agreement |
| Shape of Ossific Nucleus (Symmetric v. Eccentric) | 0.717 | 0.0001 | Substantial Agreement |
| Homogenous vs. Heterogenous Ossific Nucleus | 0.8 | 0.0001 | Substantial Agreement |
| IHDI Grade | 0.91 | 0.0001 | Near Perfect Agreement |
Cohen’s Kappa Coefficient level of agreement: ≤0=Poor, .01–.20=Slight, .21–.40=fair, .41–.60=moderate, .61–.80=substantial, and .81–1=almost perfect.
Appendix 2. Inter-Rater Reliability for Continuous Hip Measurements
| Overall Interrater Correlations | ICC | 95% CI | P Value | Level of Agreement |
|---|---|---|---|---|
| Physeal Width | 0.986 | 0.975 to 0.992 | 0.0001 | Near Perfect Agreement |
| Femoral Neck Narrowest Width | 0.98 | 0.948 to 0.993 | 0.0001 | Near Perfect Agreement |
| Subtrochanteric Shaft Width | 0.989 | 0.98 to 0.994 | 0.0001 | Near Perfect Agreement |
| Femoral Neck Length | 0.988 | 0.979 to 0.993 | 0.0001 | Near Perfect Agreement |
| Intra-trochanteric Line Length | 0.979 | 0.96 to 0.989 | 0.0001 | Near Perfect Agreement |
| Ratio of Femoral Neck Length to Intra-Trochanteric line length | 0.931 | 0.881 to 0.96 | 0.0001 | Near Perfect Agreement |
| Epiphyseal Height | 0.974 | 0.944 to 0.986 | 0.0001 | Near Perfect Agreement |
| Epiphyseal Width | 0.981 | 0.96 to 0.99 | 0.0001 | Near Perfect Agreement |
| Ratio Epiphyseal Height: Width | 0.824 | 0.503 to 0.828 | 0.0001 | Near Perfect Agreement |
| Acetabular Index | 0.741 | 0.008 to 0.903 | 0.0001 | Substantial Agreement |
| Diseased Hip Interrater Correlations | ||||
| Physeal Width | 0.98 | 0.957 to 0.991 | 0.0001 | Near Perfect Agreement |
| Femoral Neck Narrowest Width | 0.992 | 0.981 to 0.996 | 0.0001 | Near Perfect Agreement |
| Subtrochanteric Shaft Width | 0.988 | 0.974 to 0.995 | 0.0001 | Near Perfect Agreement |
| Femoral Neck Length | 0.992 | 0.981 to 0.996 | 0.0001 | Near Perfect Agreement |
| Intra-trochanteric Line Length | 0.972 | 0.933 to 0.988 | 0.0001 | Near Perfect Agreement |
| Ratio of Femoral Neck Length to Intra-Trochanteric line length | 0.933 | 0.855 to 0.97 | 0.0001 | Near Perfect Agreement |
| Epiphyseal Height | 0.983 | 0.957 to 0.994 | 0.0001 | Near Perfect Agreement |
| Epiphyseal Width | 0.98 | 0.95 to 0.992 | 0.0001 | Near Perfect Agreement |
| Ratio Epiphyseal Height: Width | 0.865 | 0.693 to 0.944 | 0.0001 | Near Perfect Agreement |
| Acetabular Index | 0.706 | 0.2 to 0.909 | 0.0001 | Substantial Agreement |
| Healthy Hip Interrater Correlations | ||||
| Physeal Width | 0.991 | 0.98 to 0.996 | 0.0001 | Near Perfect Agreement |
| Femoral Neck Narrowest Width | 0.977 | 0.841 to 0.993 | 0.0001 | Near Perfect Agreement |
| Subtrochanteric Shaft Width | 0.990 | 0.977 to 0.995 | 0.0001 | Near Perfect Agreement |
| Femoral Neck Length | 0.985 | 0.967 to 0.994 | 0.0001 | Near Perfect Agreement |
| Intra-trochanteric Line Length | 0.985 | 0.966 to 0.993 | 0.0001 | Near Perfect Agreement |
| Ratio of Femoral Neck Length to Intra-Trochanteric line length | 0.931 | 0.842 to 0.97 | 0.0001 | Near Perfect Agreement |
| Epiphyseal Height | 0.953 | 0.844 to 0.983 | 0.0001 | Near Perfect Agreement |
| Epiphyseal Width | 0.981 | 0.948 to 0.993 | 0.0001 | Near Perfect Agreement |
| Ratio Epiphyseal Height: Width | 0.688 | 0.236 to 0.871 | 0.006 | Near Perfect Agreement |
| Acetabular Index | 0.831 | 0.101 to 0.953 | 0.0001 | Near Perfect Agreement |
Intraclass Correlations (ICC) calculated based on Two Way Mixed Model with Absolute Agreement for Single Measures.