
Original Research
Appropriate Antibiotic Duration in Pediatric Bone and Joint Infection: A Systematic Review
1Department of Surgery, University of Auckland, Auckland, New Zealand; 2Department of Orthopaedic Surgery, Auckland Hospital, Auckland, New Zealand; 3Starship Children’s Hospital, Auckland, New Zealand; 4Department of Surgery, University of Auckland; 5Department of Orthopaedic Surgery, Waikato Hospital, Hamilton, New Zealand
Correspondence: Sarah Hunter, MBChB, Waikato Hospital, 183 Pembroke St., Hamilton West 3204, New Zealand. E-mail: [email protected]
Received: May 28, 2023; Accepted: September 20, 2023; Published: November 15, 2023
Volume 5, Number 4, November 2023
Abstract
Background: Optimal duration of antibiotic therapy for childhood bone and joint infection (BJI) remains controversial, despite recent literature in support of shorter courses and early oral switch. We have reviewed the literature to summarize current evidence for reduced duration of antibiotic therapy with particular attention to regional variation in pathogen type and treatment success.
Methods: Systematic review was undertaken of studies examining acute pediatric bone and joint infection over the period January 1980-December 2022 for children aged up to 18 years. Cohort studies, systematic reviews, randomized controlled trials, and prospective studies were analyzed for data on treatment success rates and duration of therapy.
Results: A total of 34 studies met inclusion criteria reporting treatment duration for 8337 cases of acute BJI. There were five prospective studies, 21 cohort studies, six randomized controlled trials, and three systematic reviews. The shortest duration of therapy tested prospectively was 10 days of combined IV and oral treatment. In the populations examined by this systematic review, there were no increased failure rates as a consequence of shorter therapy. Neonates and children with comorbid or complicated illness were routinely excluded from higher-level studies.
Conclusions: There is moderate evidence for shortened duration of therapy with early switch to oral antibiotics in select patients. Studies reporting good success for reduced therapy included healthy patients with uncomplicated disease. Regional disease variation and study protocol heterogeneity limit widespread adoption of short-course treatment. Additionally, the experience of BJI is diverse. Although the majority of children respond well to treatment, there is a subset who demonstrate acute or chronically complicated disease. Further research is needed to define patient and disease factors that contribute to treatment failure.
Level of Evidence: Systematic review Level III
Key Concepts
- In the populations examined in this systematic review, there was no evidence of increased failure rates as a consequence of shorter therapy.
- It may be reasonable to recommend short course of IV therapy with early transition to oral medication in those >3 months of age without signs of complicated disease.
- Clinicians need to be aware of regional disease variation and patient factors associated with treatment failure.
- Pathogen and genetic variability likely contribute to the success of treatment in childhood BJI.
Introduction
Childhood bone and joint infection (BJI) compromises a spectrum of disease from acute septic arthritis (SA) and acute hematogenous osteomyelitis (AHO) to disseminated osteoarticular infection.1,2 Worldwide, the most common pathogen-causing disease is Staphylococcus aureus, which has been isolated in 60-90% of culture-positive cases.3 More recently clinicians have witnessed the emergence of Kingella kingae, effectively replacing Haemophilus influenzae type b (Hib) in the vaccinated population.4 Pathogen type, disease prevalence, and outcomes vary strongly across global cohorts. Certain populations, such as Māori, Polynesian, and Aboriginal Australian children, continue to experience inequitable burden of disease.5
Empiric treatment in the 1980s comprised of prolonged inpatient intravenous (IV) antibiotic therapy and immobilization for 6 weeks.6 Despite the emergence of novel pathogens and increasing bacterial virulence, the duration of therapy has actually shortened without demonstrating higher treatment failure rates. Treatment regimens in those >3 months of age are being prospectively and retrospectively assessed to provide support for shorter therapy with early conversion to oral antibiotics.7 Potentially, this would significantly reduce the strain of disease on healthcare systems and families. However, to promote application of short-duration antibiotic therapy, there needs to be a reliable and generalizable body of evidence.
Systematic review of antibiotic duration was comprehensively undertaken by Howard-Jones et al. in 2013 with a smaller summary of evidence from Huang et al. in 2019.8,9 Huang’s analysis is thorough but includes assessment of treatment protocols for adult patients. Krzysztofiak et al. published an Italian consensus for AHO management in children based on systematic review; this comprised of a large number of studies (n=53) but included editorials, guidelines, and case series with <20 patients or subacute cases.10 This was useful in providing a broad guideline for treatment based on expert panel review; however, it lacks quality assessment for individual publications. Our research presents the most rigorous analysis of evidence up until the end of 2022, with sole focus on duration of therapy and treatment success worldwide. In the current study, we aim to answer the following question: Is shortened duration of intravenous and oral antibiotic therapy associated with higher treatment failure rates in children with AHO and/or SA?
Methods
Search Strategy
The review process was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. The goal of this search was to find publications that directly address the duration of antibiotics following diagnosis of childhood acute BJI.
The databases used were MEDLINE (Medical Literature Analysis and Retrieval System Online), CINAHL (Cumulative Index to Nursing and Allied Health Literature, Ipswich, Massachusetts), and Cochrane Library up to December 31, 2022, with date restriction to 1980. The search was conducted on January 31, 2023. Google Scholar search engine was also used to avoid missing unpublished or recently released contemporary works. The keywords for search were p(a)ediatric, ‘osteomyelitis,’ ‘septic arthritis,’ ‘antibiotics,’ ‘surgery,’ ‘bone and joint infection,’ and ‘drainage.’ Papers were excluded if they included patients >18 years, examined fewer than 20 cases, or considered only a single anatomic site. Papers focussed on chronic AHO, surgical site infection, tuberculous, reactive arthritis, or Lyme disease were also excluded.
Data Extraction
From each study, we extracted year of publication, ages and diagnosis of the study cohort, primary bacterial pathogen, geographical region, length of oral and intravenous therapy, failure rate, duration of follow-up, and primary findings reported by the authors.
Age was not reliably recorded in all studies; where an explicit age could be extracted, this is listed in Tables 1–4. However, many cohort studies only report a ‘paediatric’ study or simply describe inclusion as ‘children and infants.’
Table 1. Randomized Controlled Trials Concerning Shortened Duration of Antibiotics in Childhood BJI
| Year | Primary Author | Study Type | Inclusion | N | Age | Intervention Group | Control Group | Conclusion | GRADE Level of Evidence |
|---|---|---|---|---|---|---|---|---|---|
| 1982 | SL Kaplan13 | RCT | AHO | 25 | 1 month - 15 years | nafcillin/methicillin IV 27 days and 3.7 weeks dicloxacillin in 13 participants | IV clindamycin 5.8 days and 4.7 weeks oral clindamycin in 12 participants | 77% success rate in methicillin group, 92% success rate for clindamycin group with 6-months follow-up | Moderate |
| 1997 | H Peltola18 | Prospective RCT | S. Aureus AHO | 50 | 3 months - 14 years | Short course IV with quick transition to oral within 4 days (cephadine 150mg/kg/day) | Short course IV with quick transition to oral within 4 days (clindamycin 40mg/kg/day) | No adverse outcomes at 12-months follow-up | Moderate |
| 2002 | FM Jaberi17 | RCT | AHO + SA | 33 | <16 years | 7 days of IV therapy for SA or 10 days of IV therapy for AHO | 14 days of IV therapy for SA or 21 days of IV therapy for AHO | 100% success rate with 0.75-2.5 years follow-up | Moderate |
| 2009 | H Peltola15 | Prospective RCT | Culture positive SA | 130 | 3 months -15 years | Clindamycin or 1st generation cephalosporin for 10 days total therapy (IV for 2-4 days) | Clindamycin or first-generation cephalosporin for 30 days total therapy (IV for 2-4 days) | All patients recovered without sequelae; on late-onset infection in the 30-day group | Moderate |
| 2010 | H Peltola16 | Prospective RCT | Culture positive AHO | 131 | 3 months -15 years | Clindamycin or 1st generation cephalosporin for 20 days total therapy (IV for 2-4 days) | Clindamycin or 1st generation cephalosporin for 30 days total therapy (IV for 2-4 days) | No treatment failure in either group | I |
| 2012 | H Peltola46 | Prospective RCT | Culture positive SA + AHO | 252 | 3 months -15 years | Clindamycin or 1st generation cephalosporin for 10 days total therapy (IV for 2-4 days) regardless of SA or AHO diagnosis | Clindamycin or 1st generation cephalosporin for 30 days total therapy (IV for 2-4 days) regardless of SA or AHO diagnosis | No treatment failure at 12 months for either group | I |
Table 2. Observational Studies Examining Duration of Antibiotics in Childhood BJI
| Year of publication | Primary Author | Pathology | N | Brief Description | Region | Most common pathogen | Treatment failure rate | Follow-up | Level of Evidence |
|---|---|---|---|---|---|---|---|---|---|
| 1982 | WG Cole6 | AHO | 75 | IV inpatient therapy followed by oral outpatient therapy and immobilization for 6 weeks | Australasia | S. aureus | 5% | 2 years | IV |
| 1983 | JD Nelson19 | AHO + SA | 75 | 48 patients given cefamandole or cefuroxime IV for 5 days and transitioned to orals for 21 days once ESR/clinical picture normalized | USA | S. aureus for AHO, H. influenzae for SA | 2.6% | up to 4 months | IV |
| 1988 | GA Syrogiannopoulos20 | AHO + SA | 274 | 2-44 days of IV therapy with 1-32 days of oral therapy | USA | S. aureus for AHO, H. influenzae for SA | 3.8% | NR | IV |
| 1990 | RJ Scott21 | AHO | 116 | 2 weeks of IV therapy and up to 4 weeks oral therapy | USA | S. aureus | 0% | 3.5 months | IV |
| 1995 | A Lane-O'Kelly22 | AHO | 80 | Median IV treatment 9 days with 6 weeks total IV + oral therapy duration | Ireland | S. pyogenes | 0% | 1 year | III |
| 2002 | MB Vinod23,24 | AHO + SA | 71 | Antibiotic treatment ranged from 3.5-5.4 weeks with combination IV and oral therapy | Australia | S. aureus | 1.40% | Up to 12 months | III |
| 2007 | R Bachur24 | AHO | 29 | maximum 7 days of IV therapy; maximum 30 days combined oral + IV therapy | USA | S. aureus | 0% | 6 months | IV |
| 2009 | T Zaoutis25 | AHO | 1969 | 1021 with prolonged IV therapy and 948 with oral therapy | USA | S. aureus | 5% prolonged therapy 4% oral only | 6 months | III |
| 2015 | R Keren26 | AHO | 2060 | Post-discharge abx treatment via picc vs. oral antibiotics | USA | S. aureus | 5-6% | 6 months | III |
| 2016 | A Roul-Levy27 | AHO 'without severity criterion' | 45 | 4-day IV treatment followed by oral abx vs. oral abx only | Europe | NR | 5% oral vs. 12% IV, not statistically different | 6 months | III |
| 2016 | A Chou28 | AHO + SA | 37 | Median 11 days IV and 28 days of oral abx with CRP decline 50% at transition | Asia | S. aureus | 5% | 7 months | III |
| 2017 | J Chase McNeil29 | S. Aureus bacteremia + AHO/SA | 102 | 25 patients dc on oral and 77 patients dc on IV. | USA | S. aureus | 11-20% long-term complication rate | 45-461 days | III |
| 2012 | T Southorn30 | AHO + SA | 41 | Intravenous inpatient therapy vs. outpatient parenteral therapy | UK | NR | NR | NR | III |
| 2018 | R Quick47 | AHO + SA | 117 | 63 cases had early transition to orals after (1) confirmed dx (2) clinical improvement (3) 48h afebrile (4) 50% CRP reduction (5) minimum 72h IV | USA | S. aureus | NR | NR | III |
| 2019 | A Nielsen31 | AHO + SA | 82 | 3 days of IV therapy followed by 1 week of oral therapy in SA, three weeks of orals in AHO | Europe | S. aureus | 2% | 320 days | III |
| 2019 | A Filleron32 | AHO + SA | 176 | 48h IV therapy with minimum 15 days of total antibiotics | Europe | S. aureus | 1.2% | 1 year | |
| 2020 | S Hunter5 | SA | 2 weeks of oral followed by IV antibiotics | Australasia | S. aureus | 2.9% | 2 years | III | |
| 2021 | R. Alcobendas36 | AHO + SA | 957 | Group 1 managed with initial IV antibiotic therapy and Group 2 meeting low-risk criteria managed with oral therapy alone. Total duration of treatment ranged from 21-28 days. | Europe | S. aureus (K. kingae for those 6 months - 3 years) | 7.9% (all clinical sequelae) | 6 months | III |
| 2021 | P Musso34 | AHO | 216 | Divided into cohorts of neonatal, spondylodiscitis, and 'other' AHO | Europe | S. aureus | 3% | NR | III |
| 2021 | J Yi35 | AHO + SA | 453 | Median duration total abx therapy was 37 days for AHO and 25 days for SA or 43 days if combined. 67% received oral abx at discharge. | USA | S. aureus | 9% | NR | III |
| 2023 | S Hunter50 | AHO | 103 | All children treated with a minimum of 4-6 weeks IV antibiotics | Australasia | S. aureus | 11% | 2 years | III |
RCT (Randomised Controlled Trial); SA (Septic Arthritis); AHO (Acute Haematogenous Osteomyelitis); IV (Intravenous).
Table 3. Prospective Studies Concerning Shortened Duration of Antibiotics in Childhood BJI
| Year | Primary Author | Study Type | Inclusion | N | Age | Brief Description | Conclusion | Follow-up duration | Loss to follow up | Level of Evidence |
|---|---|---|---|---|---|---|---|---|---|---|
| 2007 | C B D Lavy37 | Prospective Cohort Study | SA | 96 | <12 | All patients receiving 6 weeks of antibiotics and interval x-rays | Radiographic change did not cease until 6 weeks | 24 weeks | 40% | II |
| 2009 | N Jagodzinski38 | Prospective Cohort Study | AHO + SA | 70 | <16 | 3-5 days of high-dose IV therapy followed by 3 weeks of oral therapy | No adverse outcomes at 1 year; 86% did not require further treatment of any kind | 1 year | NR | II |
| 2012 | M Paakkonen39 | Prospective Cohort Study | Culture positive cases of AHO + SA | 265 | 3 months - 15 years | Only 2-4 days of IV therapy; discharge defined by CRP normalization | Shortened hospital stay from median 13 to median 9 days, 1983-2005 with no change in treatment failure rate | 1 year | NR | II |
| 2014 | P Brady40 | Quality Improvement study | AHO admitted over 1 year *excluded those with comorbid conditions i.e., immunodeficiency | 31 | 3-11 years | Quality improvement intervention - cases discharged on 4-6 weeks oral abx only | No difference in treatment failure, no increase in complication rate | 6 months | NR | II |
| 2018 | R Alcobendas41 | Prospective Cohort Study | AHO + SA | 25 | <14 | Oral antibiotics only vs. intravenous for median treatment length 21 days | No complications or sequelae in the group receiving oral antibiotics alone but selection bias with pathogen (more Kingella kingae in group receiving oral only and less Staphylococcus aureus) | NR | NR | II |
RCT (Randomised Controlled Trial); SA (Septic Arthritis); AHO (Acute Haematogenous Osteomyelitis); IV (Intravenous); N (number).
Table 4. Systematic Reviews Concerning Shortened Duration of Antibiotics in Childhood BJI
| Paper | Year | N | Study type | Inclusion Criteria | Primary Outcome | Reference standard | Comparison group | Conclusion | Level of Evidence |
|---|---|---|---|---|---|---|---|---|---|
| N Le Saux42 | 2002 | 12 | Systematic review of prospective studies | Children between 3 months - 16 years with AHO. AHO dx made based on positive culture from bone or periosteum, clinical signs and blood culture, or clinical signs and positive nuclear scan or radiograph | Cure rate at 6 months | Patients receiving 1 week or longer of IV antibiotic therapy | Patients receiving 7 days of IV therapy only | Cure rate at 6 months for short-course therapy is 95.2% vs. 98.8%; no significant difference. No significant difference between oral duration of therapy | II |
| A Howard-Jones8 | 2013 | 34 | Systematic review of mixed study types | Children up to 18 years with AHO | Success rate defined as percentage of patients with radiographic resolution of lesions at follow-up and resolution of symptoms without recurrence. | Long course of IV antibiotic therapy defined as median >7 days | Short course IV therapy </= 7 days | Early transition to oral therapy in patients responding well may be as effective for longer courses. Subsequent oral therapy up to 3 weeks. Not proven in neonates | II |
| A Krzysztofiak10 | 2021 | 53 | 53 articles quoted regarding duration of antibiotics | Brief review of articles considering duration and selection of abx in children 28 days - 18 years with uncomplicated AHO (including subacute) | General summary recommendations for antibiotic type, duration, switch, and surgical vs. medical treatment | NR | NR | Discontinue oral therapy 3-5 weeks after switch if there are no complications; oral switch takes place up to 72h after the start of IV therapy if clinical condition improving | III |
RCT (Randomised Controlled Trial); SA (Septic Arthritis); AHO (Acute Haematogenous Osteomyelitis); IV (Intravenous).
Treatment failure was defined in this review as failure of first-line therapy with decision for delayed surgical intervention, secondary surgery, prolonged antibiotics >12 weeks, or chronic infection. Antibiotic selection has been noted in a brief study description but was not the focus of this review.
Quality Assessment
All publications were assigned a level of evidence according to the Journal of Bone and Joint Surgery.11 Conclusions have been summarized with strength of recommendations according to the GRADE working group.12
Results
Study Selection
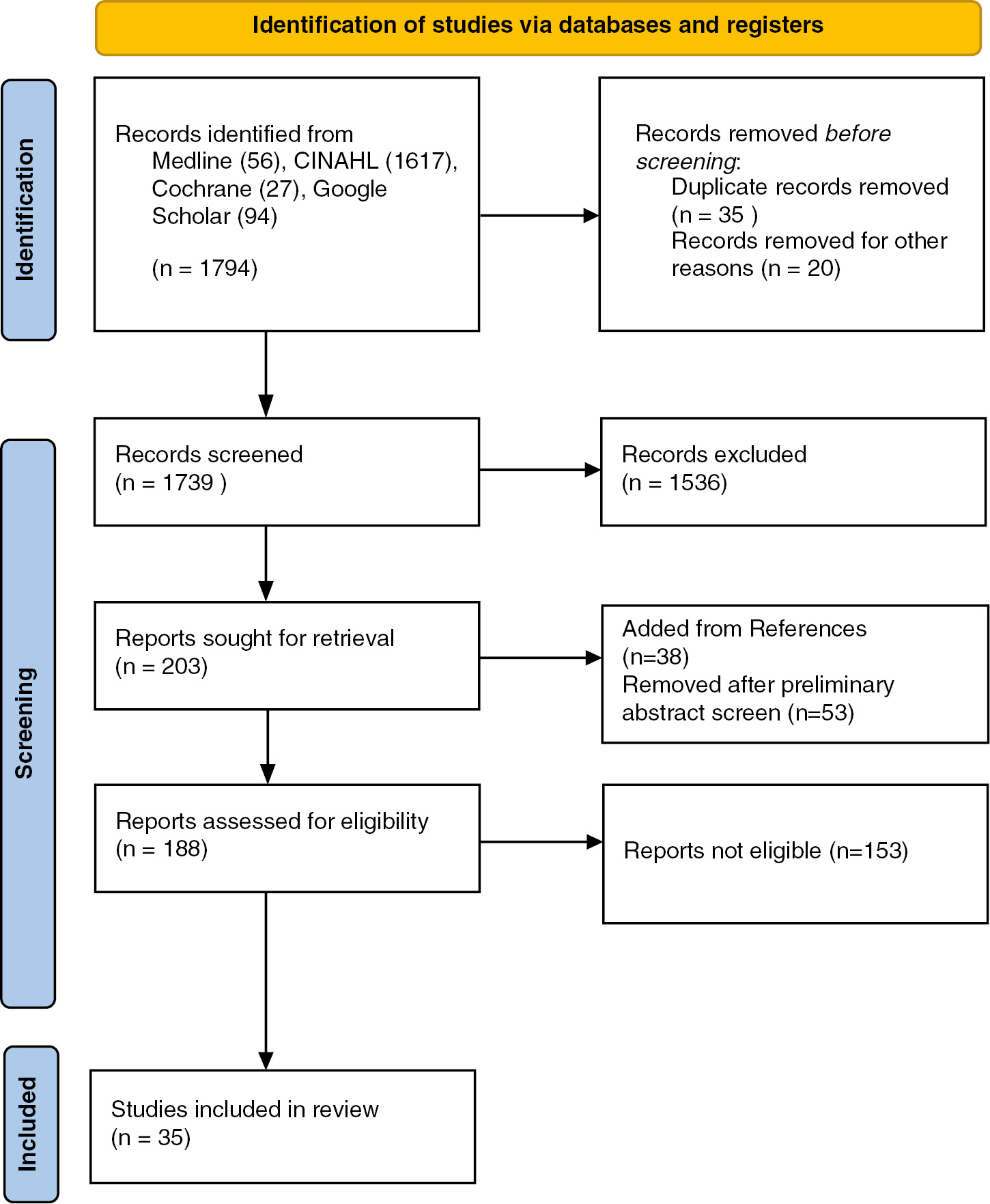
A total of 1794 citations were screened for eligibility (Figure 1). Papers not specifically reporting on antibiotic duration were excluded (n=1536). Two hundred and three papers met inclusion and exclusion criteria for initial review. Examination of publication abstracts and/or full texts led to exclusion of 53 papers and the addition of 38 research items identified in references. The final count of publications eligible for review was 188. Two reviewers (SH and HC) independently assessed each publication for inclusion.
Figure 1. PRISMA flowchart for identification of studies.
Literature review identified 35 papers meeting inclusion/exclusion criteria that address the duration of antibiotics following diagnosis of SA and/or OM. Of these papers, there were six randomized controlled trials (RCTs),13–18 21 observational studies,5–7,19–36 five prospective/quality improvement studies,37–41 and three systematic reviews.8,10,42 We have outlined the treatment success rates from each study in Tables 1–3. Systematic reviews are reported in Table 4. Some studies used in systematic reviews were excluded due to publication year prior to 1980 or sample size less than 20 participants.43–45 Two further systematic reviews were examined but not analyzed due to either inclusion of adult patients or primary focus on type of antimicrobial therapy rather than duration.9,42
Failure Rates
Treatment failure was less than 5% across all retrospective cohort studies with several notable exceptions. These were usually secondary to heterogenous definition of treatment failure. For example, the prospective study by Yi et al. had a treatment failure rate of 9%, but this included any ‘antibiotic change, new onset swelling, erythema, or pain at the original site of AHO/SA within 1 month of completing the initial antibiotic course….’ In contrast, other publications defined failure more strictly, for example, as chronic disease or re-operation within 3 months of treatment initiation.26 Notably, the studies with shortest duration of antibiotic therapy did not exhibit higher treatment failure rates.31,32
Amongst RCTs and prospective trials, the treatment success rates were high, ranging from 77-100%.14–16 The shortest duration of treatment in RCT was 30 days combined IV + oral for either AHO or SA, with no treatment failure rate documented at 12 months.14
Pathogen Type and Region
The most common pathogen across all regions was S. aureus. Three studies reported either K. kingae or H. influenzae as the dominant pathogen in toddlers.19,20,41 These studies did not report lower treatment failure. Notably, the prospective RCTs performed by Peltola et al. were conducted in populations with up to 89% methicillin-sensitive strains of S. aureus.16 Chase McNeil’s 2017 paper comments on prolonged inpatient admissions in the setting of MRSA.29 There is currently insufficient evidence to promote short-course therapy in the context of highly virulent pathogens or with severe and complicated illness.
Quality of Studies
Randomized controlled trials were assessed by the GRADE working group as moderate quality (Table 1, Appendix Table 5). Blinding was not a feature of any of these studies; a few exhibited recruitment periods >5 years.14–16
Table 2 references the quality of observational studies with regard to follow-up, treatment failure rate, and level of evidence. Within this group, a published treatment failure rate could be derived from 19/21 papers. Duration of follow-up was stated in 16/21 studies with only two reporting follow-up <6 months.
Treatment Algorithm
We propose that the following treatment algorithm (Figure 2) could be used as a guide for orthopaedic clinicians, based on the findings of this systematic review.
Figure 2. A potential treatment guide considering duration of antibiotic therapy in childhood bone and joint infection.
*Gold standard diagnostic criteria: AHO on Magnetic Resonance Imaging, Septic arthritis with organism growth on joint aspirate or intraoperative culture, or cell count from aspirate >/=50,000 WCC. *CRP resolution by 50% at day 4/5 following treatment initiation.57

Discussion
In the populations examined in this systematic review, there were no signs of increased failure rates or recurrent infections as a consequence of shorter therapy. Short courses of IV therapy for 2-4 days followed by oral antibiotics for 3-4 weeks have been assessed in retrospective, prospective, and randomized trials within the Western Organisation for Economic Development (OECD).8,15,39,42,51 This compromises the largest study to date assessing evidence for shortened antibiotic duration, including more than 8000 cases of childhood BJI. Importantly, based on the available evidence, early transition to oral therapy could be encouraged in matched populations. Children discharged on oral therapy, provided they meet specific criteria for clinical improvement, did not have worse outcomes than those who previously underwent up to 6 weeks of IV therapy in the community.3,52,53
Evolution of Treatment
Prior to 1980, only intravenous antibiotics were utilized in the treatment of acute BJI. Early observational studies in the 1980s began to explore the viability of transition to oral antibiotics while maintaining a relatively long total duration of therapy. In 1982 Cole et al. identified the possibility of shorter courses of IV therapy in OM, less than 1 week, with a transition to oral therapy and limb immobilization for a total of 6 weeks.6 The concept of transition to orals was extended to include both SA and OM by Nelson et al., who retrospectively examined 75 children receiving a median of 5 days (range 2-21 days) of IV cefamandole or cefuroxime followed by a median of 21 days oral antibiotics (range 3-84 days). Success rate was 98%.19
Moving toward a more efficient hospital experience, the largest cohort study from this period analyzed records for 274 children who were given antibiotic therapy ‘shorter than usually recommended.’20 For septic arthritis, therapies between 15-23 days did not result in recurrence over the 10-year study period. Osteomyelitis recurrence rate was around 4% after 17-24 days of treatment.
Further observational studies in the early to mid-1990s did not investigate a total treatment time of less than 6 weeks.21,22 The work of the Finnish Study Group represented the first prospective RCT for both therapy type and duration in specifically S. aureus OM.18 Comprising 50 patients, two study arms were randomized to 4 days of either cephradine or clindamycin IV, and a full treatment duration of 3-4 weeks. With 12 month follow-up there were no reports of adverse outcomes. This led to the proposition that hospital treatment for OAI in children could be greatly simplified.
A multicenter research group from Finland conducted several prospective trials looking at duration of antibiotics between 2009-2012.15,48,49 Notably, only culture-positive cases of SA or AHO were considered eligible for inclusion in these trials. The combined publications did not show significantly worsened outcomes when oral therapy was shortened to 10 (SA) or 20 (OM) days after 2-4 days of IV therapy. Hospital stay in pediatric BJI was shortened from a median of 13 to 9 days as more efficient protocols were established in these centers. Other RCTs and prospective studies from this period supported shortening treatment to less than a month for both SA and OM.17,29,38
Recently, one of the shortest durations of antibiotics trialed by an institution was at Montpellier University Hospital; 176 children received a short course antibiotic protocol where total combined treatment duration was 15 days. In this cohort, there were no treatment failures and secondary surgical revision rate was 7%.32
Outpatient Intravenous Therapy
Innovation within healthcare services has increased the availability of outpatient intravenous antibiotics via peripherally inserted central catheters (PICC). Two retrospective cohort studies of 1969 children (Zaoutis et al. 2009) and 2060 children (Keren et al. 2015) captured the introduction of prolonged outpatient IV therapy.25,26 Zaoutis et al. reviewed only cases of OM, comparing patients who received prolonged IV therapy (n=1021) and similar duration outpatient oral therapy (n=948). There was no association between treatment mode and failure or recurrence. Similarly, Keren et al. did not identify a difference between groups with regard to treatment failure. However, both studies comment on the higher readmission rate associated with PICCs and the potential disruption to patients caused by blockage or PICC-related complications. Some studies advised caution with short IV antibiotic courses in patients who have severe vertebral osteomyelitis or MRSA identified; it is probable that these factors increase risk of treatment failure.9,29
While outpatient IV therapy via PICC initially appeared to reduce morbidity, high re-admission rates for PICC-related complications have left this unattractive to clinicians.26,27,36 Early switch to oral antibiotics has the potential to significantly simplify treatment protocols and reduce PICC-related re-admissions.54 However, the potential for non-compliance with oral antibiotic treatment is higher and perhaps not captured in prospective studies where dosage and administration are closely monitored. Difficulties with compliance may be exacerbated in regions experiencing socioeconomic deprivation with reduced access to healthcare and inadequate family support.
Early Switch to Oral Antibiotics
Subsequent to 2015, several studies commented on the relationship between CRP (C-reactive protein) normalization and the ability to shorten antibiotic treatment. Chou et al. reviewed a small number of children (n=37) with AHO or SA retrospectively and noted a 97% treatment success rate if CRP declined by 50% at the time of transition from IV to oral antibiotics.28 Defining these criteria for transition further, Quick et al. suggested early change to oral antibiotics if five criteria were met: (1) a confirmed diagnosis, (2) clinical improvement, (3) afebrile for 48 hours, (4) minimum 72 hours of IV antibiotics, and (5) 50% reduction in presenting CRP.47
Limitations
Quality of evidence is an important limitation of this systematic review. At most, the randomized controlled trials presented here can be categorized as moderate grade of evidence, due to issues with blinding, limited follow-up, and prolonged recruitment.15,16 Heterogenous inclusion criteria further limit summary recommendations for childhood BJI. Most studies presented in this review exclude infants <3 months of age, have strict criteria for ‘previously healthy children,’ and produce data from OECD regions.15–17,51 Pathogen and genetic variability likely contribute to the success of treatment in childhood BJI.57 It is not recommended that treatment protocols be utilized outside the region of development without robust external validation.56
In order to make strong recommendations for shortened IV therapy and early oral transition, the definition of ‘uncomplicated’ BJI needs to be refined. This would enable a more reliable application of shortened therapy for children who will have a predictable outcome following infection. Within cohorts with AHO or SA, there remain children who experience severe disease, require extended antibiotic therapy, and undergo multiple surgeries.57 Genetic factors, socioeconomic factors, and pathogen virulence are all postulated to influence disease outcome. Finding patient and disease factors to identify the at-risk child will help to streamline care and shorten duration of treatment in the majority.
Conclusions
In conclusion, there is now an increasing body of evidence in support of shorter courses of IV and oral therapy for childhood BJI. Historic assumptions about the requirement for prolonged inpatient or even outpatient intravenous therapy are being challenged to simplify treatment protocols. It may be reasonable to recommend short course of IV therapy with early transition to oral medication in those >3 months of age without signs of complicated disease.
Disclaimer
No funding was received. The authors report no conflicts of interest related to this manuscript.
References
- Dartnell J, Ramachandran M, Katchburian M. Haematogenous acute and subacute paediatric osteomyelitis: a systematic review of the literature. J Bone Joint Surg Br. 2012;94:584-595.
- De Boeck H. Osteomyelitis and septic arthritis in children. Acta Orthop Belg. 2005;71:505-515.
- Hunter S, Chan H, Baker JF. Global epidemiology of childhood bone and joint infection: a systematic review. Infection. 2022;50(2):329-341.
- Yagupsky P. Kingella kingae: carriage, transmission, and disease. Clin Microbiol Rev. 2015;28(1):54-79.
- Hunter S, Baker JF. Ten-year retrospective review of paediatric septic arthritis in a New Zealand centre. Int Orthop. 2021;45:147-154.
- Cole W, Dalziel R, Leitl S. Treatment of acute osteomyelitis in childhood. J Bone Joint Surg Br. 1982;64:218-223.
- Quick R, Boswell P, Merkel K, et al. Impact of a pediatric evidence-based acute hematogenous osteomyelitis diagnostic and treatment algorithm. Open Forum Infect Dis. 2015;2:1510.
- Howard-Jones AR, Isaacs D. Systematic review of duration and choice of systemic antibiotic therapy for acute haematogenous bacterial osteomyelitis in children. J Paediatr Child Health. 2013;49:760-768.
- Huang CY, Hsieh RW, Yen HT, et al. Short- versus long-course antibiotics in osteomyelitis: a systematic review and meta-analysis. Int J Antimicrob Agents. 2019;53(3):246-260.
- Krzysztofiak A, Chiappini E, Venturini E, et al. Italian consensus on the therapeutic management of uncomplicated acute hematogenous osteomyelitis in children. Ital J Pediatr. 2021;47(1):179.
- Marx RG, Wilson SM, Swiontkowski MF. Updating the assignment of levels of evidence. J Bone Joint Surg Am. 2015;97(1):1-3.
- Atkins D, Eccles M, Flottorp S, et al. Systems for grading the quality of evidence and the strength of recommendations I: critical appraisal of existing approaches The GRADE Working Group. BMC Health Serv Res. 2004;4(1):38.
- Kaplan SL, Mason EO, Feigin RD. Clindamycin versus nafcillin or methicillin in the treatment of Staphylococcus aureus osteomyelitis in children. South Med J. 1982;75(2):138-142.
- Peltola H, Pääkkönen M, Kallio P, et al. Clindamycin vs. first-generation cephalosporins for acute osteoarticular infections of childhood-a prospective quasi-randomized controlled trial. Clin Microbiol Infect. 2012;18(6):582-589.
- Peltola H, Pääkkönen M, Kallio P, et al. Prospective, randomized trial of 10 days versus 30 days of antimicrobial treatment, including a short-term course of parenteral therapy, for childhood septic arthritis. Clin Infect Dis. 2009;48(9):1201-1210.
- Peltola H, Pääkkönen M, Kallio P, et al. Short-versus long-term antimicrobial treatment for acute hematogenous osteomyelitis of childhood: prospective, randomized trial on 131 culture-positive cases. Pediatr Infect Dis J. 2010;29:1123-1128.
- Jaberi FM, Shahcheraghi GH, Ahadzadeh M. Short-term intravenous antibiotic treatment of acute hematogenous bone and joint infection in children: a prospective randomized trial. J Pediatr Orthop. 2002;22:317-320.
- Peltola H, Unkila-Kallio L, Kallio MJT, et al. Simplified treatment of acute staphylococcal osteomyelitis of childhood. Pediatrics. 1997;99:846-850.
- Nelson JD, Bucholz RW, Kusmiesz H, et al. Benefits and risks of sequential parenteral-oral cephalosporin therapy for suppurative bone and joint infections. J Pediatr Orthop. 1982;2:255-262.
- Syrogiannopoulos GA, Nelson JD. Duration of antimicrobial therapy for acute suppurative osteoarticular infections. Lancet. 1988;1:37-40.
- Scott RJ, Christofersen MR, Robertson WW, et al. Acute osteomyelitis in children: a review of 116 cases. J Pediatr Orthop. 1990;10(5):649-652.
- Lane-O’Kelly A, Moloney AC. Acute haematogenous osteomyelitis — evaluation of management in the 1990s. Ir J Med Sci. 1995;164:285-288.
- Vinod M, Matussek J, Curtis N, et al. Duration of antibiotics in children with osteomyelitis and septic arthritis. J Paediatr Child Health. 2002;38(4):363-367.
- Bachur R, Pagon Z. Success of short-course parenteral antibiotic therapy for acute osteomyelitis of childhood. Clin Pediatr (Phila). 2007;46(1):30-35.
- Zaoutis T, Localio AR, Leckerman K, et al. Prolonged intravenous therapy versus early transition to oral antimicrobial therapy for acute osteomyelitis in children. Pediatrics. 2009;123:636-642.
- Keren R, Shah SS, Srivastava R, et al. Comparative effectiveness of intravenous vs oral antibiotics for postdischarge treatment of acute osteomyelitis in children. JAMA Pediatr. 2015;169:120-128.
- Roul-Levy A, Looten V, Bachy M, et al. Oral ambulatory treatment of acute osteomyelitis in children. Pediatr Emerg Care. 2016;32(3):154-156.
- Chou ACC, Mahadev A. Acute bacterial osteomyelitis in children. J Orthop Surg. 2016;24:250-252.
- Chase McNeil J, Kaplan SL, Vallejo JG. The influence of the route of antibiotic administration, methicillin susceptibility, vancomycin duration and serum trough concentration on outcomes of pediatric staphylococcus aureus bacteremic osteoarticular infection. Pediatr Infect Dis J. 2017;36:572-577.
- Southorn T, Tharmarajah P, Rehm A, et al. Outpatient Treatment of Paediatric Septic Arthritis and Osteomyelitis. American Academy of Paediatrics; 2012.
- Nielsen AB, Nygaard U, Hoffmann T, et al. Short individualised treatment of bone and joint infections in Danish children. Arch Dis Child. 2019;104:205-206.
- Filleron A, Laurens ME, Marin G, et al. Short-course antibiotic treatment of bone and joint infections in children: a retrospective study at Montpellier University Hospital from 2009 to 2013. J Antimicrob Chemother. 2019;74:3579-3587.
- Hunter S, Crawford H, Baker JF. Ten-year review of acute pediatric hematogenous osteomyelitis at a New Zealand tertiary referral center. J Pediatr Orthop. 2023;43:e396-e401.
- Musso P, Parigi S, Bossi G, et al. Epidemiology and management of acute hematogenous osteomyelitis, neonatal osteomyelitis and spondylodiscitis in a third level paediatric center. Children. 2021;8(8):616.
- Yi J, Wood JB, Creech CB, et al. Clinical epidemiology and outcomes of pediatric musculoskeletal infections. J Pediatr. 2021;234:236-244.e2.
- Alcobendas Rueda RM, Núñez E, Martín L, et al. Oral versus intravenous antibiotics for pediatric osteoarticular infection: when and to whom? Pediatr Infect Dis J. 2022;41(9):e351-e357.
- Lavy CBD, Thyoka M. For how long should antibiotics be given in acute paediatric septic arthritis? A prospective audit of 96 cases. Trop Doct. 2007;37(4):195-197.
- Jagodzinski NA, Kanwar R, Graham K, et al. Prospective evaluation of a shortened regimen of treatment for acute osteomyelitis and septic arthritis in children. J Pediatr Orthop. 2009;29(5):518-525.
- Pääkkönen M, Peltola H. Antibiotic treatment for acute haematogenous osteomyelitis of childhood: moving towards shorter courses and oral administration. Int J Antimicrob Agents. 2011;38:273-280.
- Brady PW, Brinkman WB, Simmons JM, et al. Oral antibiotics at discharge for children with acute osteomyelitis: a rapid cycle improvement project. BMJ Qual Saf. 2014;23(6):499-507.
- Alcobendas R, Remesal A, Murias S, et al. Outpatients with acute osteoarticular infections had favourable outcomes when they received just oral antibiotics without intravenous antibiotics. Acta Paediatr. 2018;107(10):1792-1797.
- Le Saux N, Howard A, Barrowman NJ, et al. Shorter courses of parenteral antibiotic therapy do not appear to influence response rates for children with acute hematogenous osteomyelitis: a systematic review. BMC Infect Dis. 2002;2:16.
- Gillespie WJ. Racial and environmental factors in acute haematogenous osteomyelitis in New Zealand. N Z Med J. 1979;90(641):93-95.
- Gillespie W, Mayo K. The management of acute haematogenous osteomyelitis in the antibiotic era: a study of the outcome. J Bone Joint Surg Br. 1981;63-B(1):126-131.
- Dich VQ. Osteomyelitis in infants and children. Am J Dis Child. 1975;129(11):1273-1278.
- Pääkkönen M, Kallio MJT, Kallio PE, et al. Shortened hospital stay for childhood bone and joint infections: analysis of 265 prospectively collected culture-positive cases in 1983–2005. Scand J Infect Dis. 2012;44(9):683-688.
- Quick RD, Williams J, Fernandez M, et al. Improved diagnosis and treatment of bone and joint infections using an evidence-based treatment guideline. J Pediatr Orthop. 2018;38(6):e354-e359.
- Pääkkönen M, Peltola H. Treatment of acute septic arthritis. Pediatr Infect Dis J. 2013;32(6):684-685.
- Pääkkönen M, Kallio PE, Kallio MJT, et al. Management of osteoarticular infections caused by staphylococcus aureus is similar to that of other etiologies: analysis of 199 staphylococcal bone and joint infections. Pediatr Infect Dis J. 2012;31:436-438.
- Hunter S, Baker JF. Quality of life in children up to 13 years following acute haematogenous osteomyelitis. J Pediatr Orthop B. 2023;32:490-496.
- Pääkkönen M, Peltola H. Simplifying the treatment of acute bacterial bone and joint infections in children. Expert Rev Anti Infect Ther. 2011;9:1125-1131.
- Pääkkönen M, Peltola H. Bone and joint infections. Pediatr Clin North Am. 2013;60:425-436.
- Iliadis AD, Ramachandran M. Paediatric bone and joint infection. EFORT Open Rev. 2017;2:7-12.
- Street M, Puna R, Huang M, et al. Pediatric acute hematogenous osteomyelitis. J Pediatr Orthop. 2015;35:634-639.
- Xie X, Li J, Gu F, et al. Genetic determinants for bacterial osteomyelitis: a focused systematic review of published literature. Front Genet. 2021;12:654792.
- Hunter S, Kennedy J, Baker JF. External validation of an algorithm to predict adjacent musculoskeletal infection in pediatric patients with septic arthritis. J Pediatr Orthop. 2020;40(10):e999-e1004.
- Hunter S, Baker JF. Early CRP trends in childhood osteomyelitis predict complicated disease. J PediatrOrthop. 2023;43(1):e74-e79.
Appendix
Table 5. Quality Assessment for Randomized Controlled Trials Concerning Antibiotic Duration
| Year of publication | Primary author | No patient blinding | No clinician blinding | No assessor blinding | Sample size <30 | Loss to FU >20% | Prolonged recruitment >5 years | Outcomes not well described | GRADE of evidence |
|---|---|---|---|---|---|---|---|---|---|
| 1982 | SL Kaplan13 | NR | NR | NR | ✔ | ✔ | / | / | Moderate |
| 1997 | H Peltola18 | NR | NR | NR | / | ✔ | / | / | Moderate |
| 2002 | FM Jaberi17 | ✔ | ✔ | NR | ✔ | / | ✔ | / | Moderate |
| 2009 | H Peltola15 | ✔ | ✔ | NR | / | / | ✔ | / | Moderate |
| 2010 | H Peltola16 | ✔ | ✔ | NR | / | / | ✔ | / | Moderate |
| 2012 | H Peltola14 | ✔ | ✔ | NR | / | / | ✔ | / | Moderate |
NR (Not Reported); FU (Follow-Up).