
Invited Perspective
What’s New in Orthopaedic Management in Neuromuscular Disorders
Shriners Children’s Hospital–Northern California, University of California Davis, Sacramento, CA
Correspondence: Amanda T. Whitaker, MD, University of California Davis, 4860 Y St., Suite 3800, Sacramento, CA 95817. E-mail: [email protected]
Received: May 24, 2022; Accepted: June 22, 2022; Published: August 1, 2022
DOI: 10.55275/JPOSNA-2022-0072
Volume 4, Number 3, August 2022

Overview
Over 6,000 articles were published in the neuromuscular space from 2021-2022. In this manuscript, we seek to review the influential papers covering the spectrum of neuromuscular orthopaedics as well as to highlight important points from presentations during Neuromuscular Subspecialty Day at POSNA on May 12, 2022, and other orthopaedic meetings in 2022. This material will hopefully inspire potential changes in our practice in the future.
We Live in a Changing World
Advances in maternal and perinatal care in Europe and Australia have led to a decrease in prenatal and perinatal cerebral palsy.1–3 The decrease may change the landscape of cerebral palsy care. Prenatal and perinatal cerebral palsy is often associated with higher proportion of spastic diplegic cerebral palsy and higher Gross Motor Functional Classification System (GMFCS) levels (IV and V). Cerebral palsy occurring in full-term children tends to have a more dyskinetic subtype and more ambulatory children (GMFCS I-III). Also, full-term children with cerebral palsy have a higher association with maternal obesity. Maternal obesity in the United States is now estimated to be over 29%, with significant racial and socioeconomic differences.4,5 For the United States, there are no recent publications illustrating a decrease in prenatal and perinatal cerebral palsy incidence. Based on existing disparities in medical care, however, the quality of maternal care may result in different trends with regard to race and socioeconomic status in the incidence and distribution of cerebral palsy.6
In 2022, we remain in the COVID-19 pandemic while trying to continue care for children with neuromuscular conditions. Respiratory syncytial virus (RSV) and other pulmonary viruses are notorious for causing devastating illnesses in our medically fragile patients.7 COVID-19 was feared to have the same, devastating effects; however, that does not appear to be true. Very few deaths have been attributed to COVID-19 in children with cerebral palsy, SMA, Duchenne’s Muscular Dystrophy, and other neuromuscular conditions.8,9
While telehealth has changed the landscape of our orthopaedic surgery clinics, the need to physically see, examine, and radiograph our patients is critical to monitor for hip subluxation, gait deterioration, and scoliosis progression. Children with cerebral palsy have a high no-show rate, especially in orthopaedic clinics (14.8%).10 This rate of missed appointments was not due to travel distance, higher GMFCS level, increased comorbidities, or a recent multidisciplinary clinic visit. The highest prediction elements of missing a clinic visit for a child with cerebral palsy are a recent reschedule or cancellation, previous no-show, socioeconomic disadvantage, and children ages 5-14 years old. These risk factors can be used to help further identify barriers to help our families have consistent follow-up and optimize clinic utilization.
Anesthesia Considerations
The preparation of children with cerebral palsy to undergo anesthesia is a careful process that is not without risk. Children with cerebral palsy require increased doses of the paralytic rocuronium.11 In a prospective study, it is noted higher GMFCS level, higher birth weight, and full-term gestational age need a larger amount of rocuronium for neuromuscular blockade. This is likely due to the disruption of the neuromuscular junctions.11
Regional anesthesia has gained popular acceptance for lower extremity surgery to decrease opioids in the perioperative period. Many children with cerebral palsy undergoing bilateral hip reconstructive surgery have baclofen pumps, which may be a contraindication for epidural anesthesia. However, two small studies have been published using epidurals in children with intrathecal baclofen pumps with successful analgesia, no infections, and no disruptions of the pumps.12,13
It remains unknown whether neuraxial analgesia or a peripheral nerve block is the most effective for pain control. Two studies presented at the 2022 Pediatric Orthopaedic Society of North America (POSNA) Annual Meeting suggested either fascia iliaca or lumbar plexus blocks may be more effective.14,15 One of the studies on baclofen pumps suggested an epidural was more effective than a lumbar plexus block.13 More work is needed for the mechanism of optimal delivery of safe and effective pain management for patients undergoing hip reconstruction and single-event multilevel surgeries (SEMLs).
In Charcot-Marie Tooth, there is a concern for further nerve damage with the use of perioperative peripheral nerve blocks for pain relief. In a retrospective review, 53 patients underwent 132 regional blocks with no evidence of neurologic complications or nerve injury related to the block.16 A prospective study of 20 patients with 24 peripheral nerve catheters for foot surgeries found no new nerve deficits after surgery and improved pain control compared to their previous methods.17 These studies suggest that peripheral nerve blocks may not cause further verve damage in Charcot-Marie Tooth foot reconstructions and may have a benefit for effective pain management.
Cast Complications
Cast problems in children with neuromuscular conditions were presented at the 2022 American Academy of Orthopaedic Surgery (AAOS) Annual Meeting.18 They found 14/28 cast injuries were in children with a neuromuscular diagnosis and all were pressure ulcers. There was no difference in who placed the cast (attending surgeon, resident, or cast tech) or where the cast was placed (operating room, clinic, or emergency room). Children with a neuromuscular diagnosis have a 40% increased risk of cast injury. This is a humbling paper of preventable risk, reminding us to stay diligent with increased padding and better molding in our high-risk patients.19
How Do We Prevent Hip Subluxation after Reconstruction Surgery in Patients with CP?
Much of the work published this past year on hip surgery in cerebral palsy involved how to prevent hip subluxation or dislocation after their initial hip surgery. Children at higher risk of severe subluxation or revision surgery are those under 6 years old, who have a worse preoperative migration percentage, and who have had only a proximal femoral varus derotation osteotomy at the time of their initial surgery.20 Adding a pelvic osteotomy had a better postoperative migration percentage, and no hips with a pelvic osteotomy underwent a revision or had a severe subluxation at a 2-year follow-up.20 This work was supported by another single-center retrospective review suggesting increased failure at an age less than or equal to 6 years old, a preoperative migration percentage of greater than 70%, or a preoperative neck-shaft angle of greater than 150 degrees at the time of neuromuscular hip reconstruction increased risk of failure.21 Those that did not have a migration percentage >50% or a revision surgery at a 2-year follow-up had more pelvic osteotomies at their initial surgery or a preoperative acetabular index of less than 25 degrees.21 While not all the above studies looked at their postoperative results, they suggest that more coverage, by adding a pelvic osteotomy, decreases future hip revision surgery. The concept of “over-containment,” defined as a migration percentage <0%, was examined by Zakrzewski et al.22 By over-containing the hips, the incidence of a migration percentage >30% or revision surgery in children with a GMFCS of IV or V, less than 6-years-old at the time of hip surgery, or a migration percentage of greater than 50% at the time of surgery all decreased.22
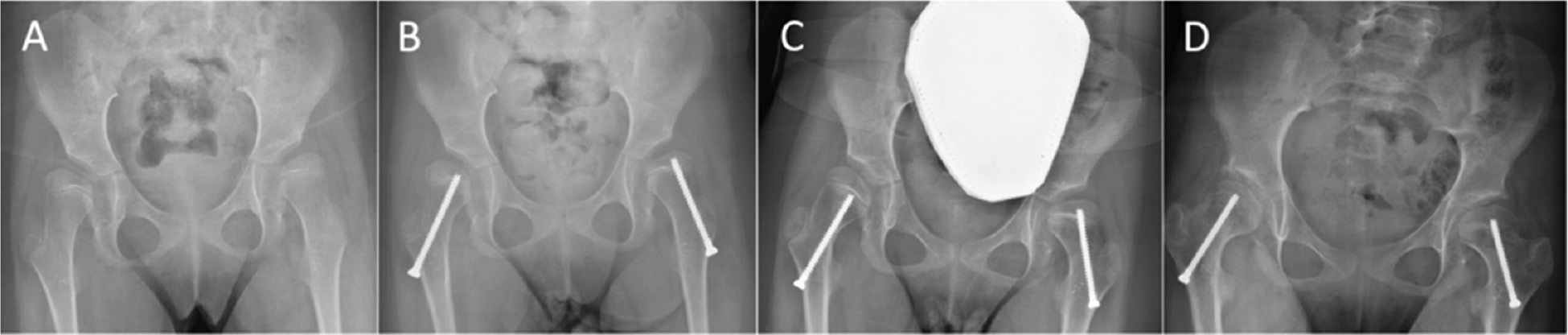
There was a lively debate on guided growth of the femoral head at POSNA this year between Jon Davids, MD, from Shriners Children’s Hospital Northern California, and Vineeta Swaroop, MD, from Lurie Children’s Hospital of Chicago (Figure 1). The results of the debate and case discussions highlighted the need for further long-term research on who is a candidate and when the procedure is appropriate. Shedding light on this subject was a paper published out of Cincinnati Children’s Hospital with a 2-year follow-up of 44 hips that underwent proximal femoral screw hemiepiphysiodesis.23 In this group, those that previously had surgery had no progression of their hip subluxation. There were improvements in migration percentage in the children who did not have prior hip reconstructive surgery; however, four hips did undergo reconstructive hip surgery in this group after their proximal femoral hemiepiphysiodesis.23
Figure 1. A) A 5-year-old with bilateral hip subluxation (right migration 50%, left migration 40%). B) At 6-yearsold after bilateral proximal femoral guided growth. C) At age 9 with disengagement of the right screw from the epiphysis. D) At age 12 after revision of the right screw (right migration 20%, left migration 20%). Images courtesy of Jon Davids, MD.
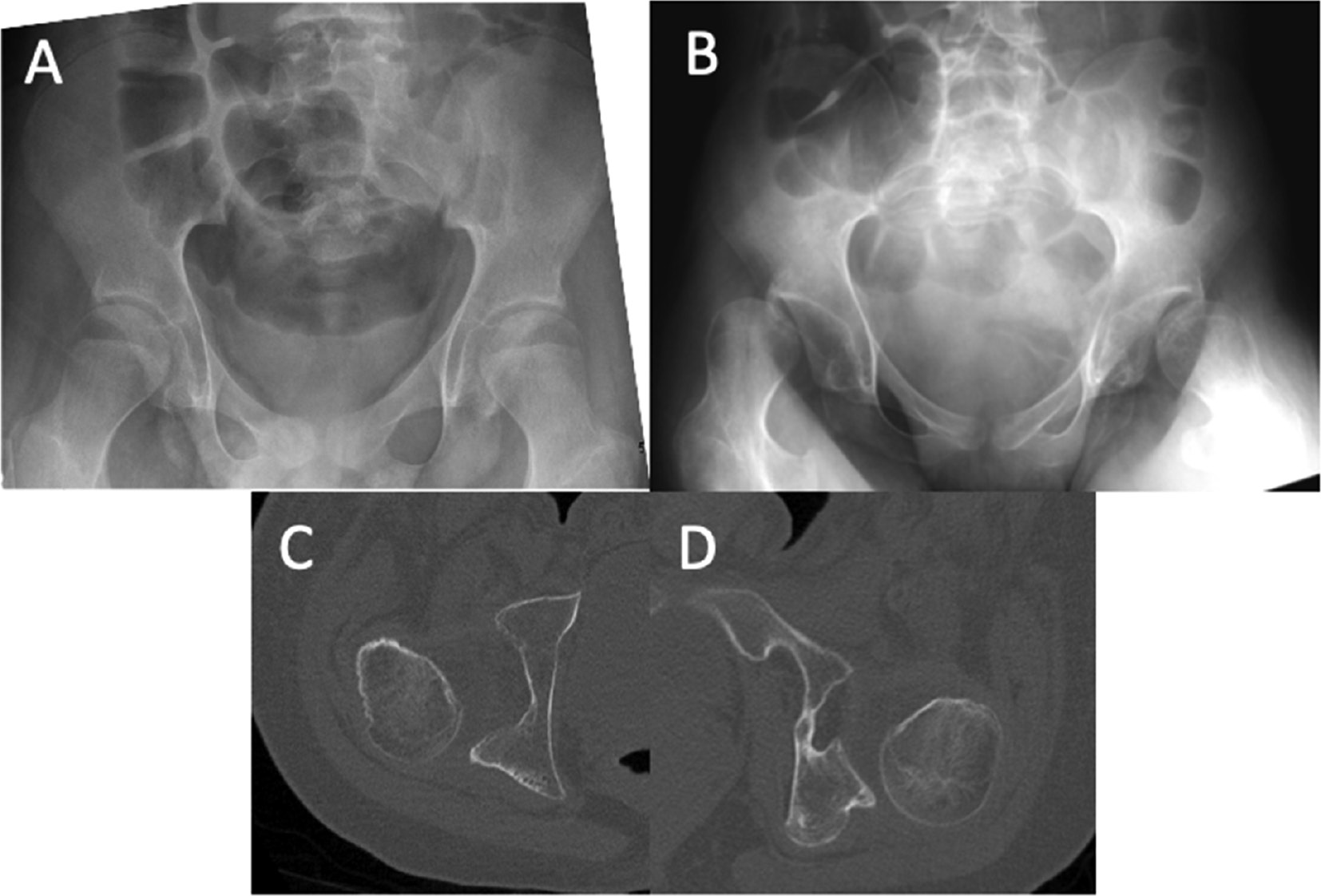
Future research and clinical decisions are impaired based on the variable definition of “failure” of hip reconstruction in the literature. Some use a migration percentage of >50%, others >30%. Data was presented at POSNA this year suggesting a migration percentage of 35% or greater at skeletal maturity can lead to further hip subluxation/dislocation into adulthood (Figure 2).24 This migration percentage is lower than was previously believed to be a “stable” hip at skeletal maturity. Another area of high variability is the varied postoperative immobilization techniques and protocols among surgeons.25
The recovery from hip reconstruction and spine surgery is painful, with short-term improvements in Health Related Quality of Life (HRQoL) and caregiver burden.26 After 5 years, the improvement in HRQoL and caregiver burden is maintained after hip reconstruction but declines to pre-surgical baseline after spine fusion.27 The natural history of cerebral palsy is a decline in function and GMFCS with time, so maintenance of pre-surgical HRQoL may be an improvement based on natural history, however, the natural history in a matched cohort is not available.28,29
Figure 2. A) 14-year-old with GMFCS IV cerebral palsy, right migration 25% and left migration 20%. B) At age 18 with bilateral severe posterior subluxation on x-ray and CT scan of the C) right hip and D) left hip.
Spine
There is new information regarding neuromuscular scoliosis mortality and infections. A large multicenter review of children with early-onset neuromuscular scoliosis demonstrated a low mortality rate at 2-year follow-up (1.1%).30 However, at 10 years, the mortality rate was 17.4%, with a 33.8% mortality rate in children with cerebral palsy.30 This data suggests that it is not the surgery, but the underlying neuromuscular condition, that increases the child’s risk for mortality. We lack an ethical control group to be able to accurately interpret the results.
The use of vancomycin powder and the adoption of surgical site infection bundles have decreased infections in spine surgery.31–34 The most common infectious organisms in children with cerebral palsy who have a postoperative spine infection are gram-negative rods and polymicrobial infections. However, children who had vancomycin powder at the time of their initial surgery had a higher rate of Proteus infections.35 Thus, the use of vancomycin powder may be changing the typical bacteria present in postoperative infections.
Treatment of Gait Abnormalities in CP
How to treat a stiff knee gait is frequently debated. McCarthy et al. and “Mission I’m Possible” have used Delphi techniques to improve decision-making and future research questions around gait-changing lower extremity surgery in children with cerebral palsy.36–38 This year, in the literature, the debate and uncertainty continued. When and how to address stiff knee gait through rectus femoris surgery was the topic of the latest Delphi analysis.37 Consensus was achieved for some indications for rectus femoris surgery, such as decreased peak knee flexion and extension with a delay in peak knee flexion and GMFCS I/II. In addition, distal lengthening was preferred over proximal lengthening of the recuts femoris if lengthening was indicated. However, a consensus was not obtained on what type of rectus femoris surgery (transfer versus lengthening) or what the most important kinematic outcome is after surgery.37 To support the lack of consensus on whether to do a recuts femoris transfer or a rectus femoris lengthening, Salazar-Torres et al. published their retrospective results of rectus femoris transfer or lengthening with at least 1-year follow-up with instrumented gait analysis.39 Both groups improved their peak knee flexion in swing; however, those with GMFCS III/IV cerebral palsy had more crouch with the rectus transfer. Crouch was not found in the rectus femoris lengthening group.39 The groups were not matched, as more children in the transfer group had concomitant hamstring lengthenings and more bilateral procedures, adding fuel to further debate on the indications and type of procedure for a stiff knee gait.
There is a hope in cerebral palsy that if spasticity is the driver of all deformities and musculoskeletal issues, then if spasticity is eliminated, orthopaedic surgical interventions can be eliminated or reduced.40 A multicenter, retrospective matched cohort study examined children with and without a selective dorsal rhizotomy with greater than 10-year follow-up.41 Children who had a selective dorsal rhizotomy had decreased spasticity at 10 years, however, underwent more orthopaedic surgeries. To date, this is the best and most comprehensive level III evidence of the musculoskeletal outcomes after selective dorsal rhizotomy (SDR) and subsequent orthopaedic surgeries with and without SDR.
We all have heard “Nothing ruins a good surgical outcome like long-term follow-up.” Boyer et al. published their long-term functional outcomes after femoral derotation osteotomy compared to those with instrumented gait analysis and femoral anteversion who did not undergo a femoral derotation osteotomy.42 Despite a 29 degree difference in femoral rotation, there was no change in their long-term functional outcomes. The derotation group reported more tripping and falling than the control group. This raises the question of the importance of restoring the hip abductor moment arm in femoral anteversion in cerebral palsy.
Similar to decreases in success in hip surgery, younger children who undergo plantarflexor lengthening surgery often have recurrence of their equinus. In a single-center retrospective review, 44% of children under the age of 7 at the time of their gastrocnemius soleus fascial lengthening or were a GMFCS III had recurrent equinus requiring a revision.43 This can assist in counseling children and families in the rate of recurrence after surgery.
Deep Vein Thrombosis in CP?
With large lower extremity surgery, whether hip reconstruction or SEMLs surgery, there are often questions about deep vein thrombosis (DVT) prophylaxis after surgery. Sees et al. reported their single-center retrospective review of 2,583 surgeries in 1,371 patients.44 They found six DVTs within 3 months of surgery. Of the six with postoperative DVTs, five of those had a coagulopathy and only three were in the lower extremities. This reinforces no routine mechanical or chemoprophylaxis for DVT prophylaxis in children with cerebral palsy undergoing hip reconstruction or SEMLs and a careful history discussing bleeding/clotting disorders preoperatively.
Conclusion
Many important studies have been published and presented in the neuromuscular orthopaedics in the past year. The demographics of cerebral palsy may be changing and creating further disparities in our healthcare system. Authors and presenters are to be congratulated for moving the bar forward on how we can better care for our patients, be more effective with our surgeries, and improve the long-term outcomes in our adult patient populations.
Disclaimer
The author has no conflicts of interest to report.
References
- Arnaud C, Ehlinger V, Delobel-Ayoub M, et al. Trends in prevalence and severity of pre/perinatal cerebral palsy among children born preterm from 2004 to 2010: A SCPE Collaboration Study. Front Neurol. 2021;12:624884.
- Smithers-Sheedy H, Waight E, Goldsmith S, et al. Declining trends in birth prevalence and severity of singletons with cerebral palsy of prenatal or perinatal origin in Australia: a population-based observational study. Dev Med Child Neurol. Published online March 8, 2022:dmcn. Epub ahead of print.
- Villamor E. Changing trends in cerebral palsy prevalence: an opportunity to consider etiological pathways. Dev Med Child Neurol. Published online March 23, 2022:dmcn.15223. Epub ahead of print.
- Tong L, Kalish BT. The impact of maternal obesity on childhood neurodevelopment. J Perinatol. 2021;41(5):928–939.
- Driscoll AK, Gregory ECW. Increases in prepregnancy obesity: United States, 2016–2019. NCHS Data Brief, no 392. Hyattsville, MD: National Center for Health Statistics. 2020.
- Flanagan D, Gaebler D, Bart-Plange ELB, et al. Addressing disparities among children with cerebral palsy: Optimizing enablement, functioning, and participation. J Pediatr Rehabil Med. 2021;14(2):153-159.
- Welliver RC, Checchia PA, Bauman JH, et al. Fatality rates in published reports of RSV hospitalizations among high-risk and otherwise healthy children. Curr Med Res Opin. 2010;26(9):2175-2181.
- Natera-de Benito D, Aguilera-Albesa S, Costa-Comellas L, et al. COVID-19 in children with neuromuscular disorders. J Neurol. 2021;268(9):3081-3085.
- Williamson EJ, McDonald HI, Bhaskaran K, et al. Risks of covid-19 hospital admission and death for people with learning disability: population based cohort study using the OpenSAFELY platform. BMJ. 2021;374:n1592.
- Paget SP, McIntyre S, Goldsmith S, et al. Non-attendance at outpatient clinic appointments by children with cerebral palsy. Dev Med Child Neurol. Published online March 4, 2022. Epub ahead of print.
- Lee S, Robinson K, Lodge M, et al. Resistance to neuromuscular blockade by rocuronium in surgical patients with spastic cerebral palsy. JPM. 2021;11(8):765.
- Kulkarni VA, Kephart DT, Ball MA, et al. Neuraxial anesthesia for post-operative pain control after hip surgery in children with cerebral palsy and pre-existing intrathecal baclofen pumps. J Pediatr Rehabil Med. 2022;15(1):3-11.
- Samineni AV, Eklund SE, Miller PE, et al. Epidural analgesia versus lumbar plexus blockade after hip reconstruction surgery in children with cerebral palsy and intrathecal baclofen pumps: a comparison of safety and efficacy. J Pediatr Orthop. 2022;42(4):222-228.
- Laron D, Kelley J, Chidambaran V, et al. Fascia iliaca pain block results in lower overall opioid usage and shorter hospital stays than epidural anesthesia after hip reconstruction in children with cerebral palsy. J Pediatr Orthop. 2022;42(2):96-99.
- Trionfo A. Lumbar plexus nerve blocks for perioperative pain management in cerebral palsy patients undergoing hip reconstruction: more effective than general anesthesia and epidurals. Presented at: Pediatric Orthopaedic Society of North America; May 12, 2022; Vancouver, BC, Canada.
- McClain RL, Rubin DI, Bais KS, et al. Regional anesthesia in patients with Charcot–Marie–Tooth disease: a historical cohort study of 53 patients. Can J Anesth. 2022;69(7):880-884.
- An T, Schwartz E, Kissen M, et al. Safety and efficacy of postoperative indwelling popliteal nerve catheters for outpatient charcot-marie-tooth surgery. Foot Ankle Int. 2022;43(4):504-508.
- Lin AJ, Cao LA, Lightdale-Miric N, et al. Neuromuscular patients are 40% more likely to get a cast injury. J Pediatr Orthop. 2022;42(3):144-148.
- Murgai RR, Compton E, Patel AR, et al. Foam padding in postoperative lower extremity casting: an inexpensive way to protect patients. J Pediatr Orthop. 2018;38(8):e470-e474.
- Bean BK, Baird GO, Caskey PM, et al. Early bony hip reconstructive surgery for hip subluxation in children with severe cerebral palsy. Orthopedics. 2021;44(2):e294-e300.
- Minaie A, Gordon JE, Schoenecker P, et al. Failure of hip reconstruction in children with cerebral palsy: what are the risk factors? J Pediatr Orthop. 2022;42(1):e78-e82.
- Zakrzewski AM, Bryant AJ, McCarthy JJ. Can over-containment prevent recurrence in children with cerebral palsy and hip dysplasia undergoing hip reconstruction? J Pediatr Orthop. 2022;42:300-306.
- Zakrzewski AM, Carl JR, McCarthy JJ. Proximal femoral screw hemiepiphysiodesis in children with cerebral palsy improves the radiographic measures of hip subluxation. J Pediatr Orthop. 2022;42:e583-e589.
- Howard J. Progression of hip displacement after triradiate cartilage closure in non-ambulatory cerebral palsy (CP): who needs continued radiographic surveillance? Presented at: Pediatric Orthopaedic Society of North America; May 12, 2022; Vancouver, BC, Canada.
- Miller SD, Juricic M, Fajardo N, et al. Variability in postoperative immobilization and rehabilitation following reconstructive hip surgery in nonambulatory children with cerebral palsy. J Pediatr Orthop. 2021;41:e563-e569.
- DiFazio R, Shore B, Vessey JA, et al. Effect of hip reconstructive surgery on health-related quality of life of non-ambulatory children with cerebral palsy. J Bone Joint Surg Am. 2016;98(14):1190-1198.
- DiFazio RL, Vessey JA, Miller PE, et al. Health-related quality of life and caregiver burden after hip reconstruction and spinal fusion in children with spastic cerebral palsy. Dev Med Child Neurol. 2022;64(1):80-87.
- Bottos M, Feliciangeli A, Sciuto L, et al. Functional status of adults with cerebral palsy and implications for treatment of children. Dev Med Child Neurol. 2001;43(8):516-528.
- Hanna SE, Rosenbaum PL, Bartlett DJ, et al. Stability and decline in gross motor function among children and youth with cerebral palsy aged 2 to 21 years. Dev Med Child Neurol. 2009;51(4):295-302.
- Matsumoto H, Fano AN, Herman ET, et al. Mortality in neuromuscular early onset scoliosis following spinal deformity surgery. J Pediatr Orthop. 2022;42(3):e234-e241.
- Partridge E, Blumberg D, Roberto RF. Prevention of spinal fusion post-operative wound infections in pediatric patients with scoliosis: a quality improvement initiative. Spine Deform. 2021;9(4):955-958.
- Roberto RF, Rowan FA, Nallur D, et al. Povidone-iodine irrigation combined with Vancomycin powder lowers infection rates in pediatric deformity surgery. Spine Deform. 2021;9(5):1315-1321.
- Hammoor B, Matsumoto H, Marciano G, et al. Surgical site infections in pediatric spinal surgery after implementation of a quality assurance program. Spine Deform. 2021;9(1):125-133.
- Stephan SR, Illingworth KD, Gupta K, et al. Surgical site infection following neuromuscular posterior spinal fusion fell 72% after adopting the 2013 best practice guidelines. Spine (Phila Pa 1976). 2021;46(17):1147-1153.
- Du JY, Dumaine AM, Klyce W, et al. Use of Vancomycin powder in spinal deformity surgery in cerebral palsy patients is associated with proteus surgical site infections. J Pediatr Orthop. 2022;42(5):280-284.
- McCarthy J, Wade Shrader M, Graham K, et al. Establishing surgical indications for hamstring lengthening and femoral derotational osteotomy in ambulatory children with cerebral palsy. J Child Orthop. 2020;14(1):50-57.
- Kay RM, Pierz K, McCarthy J, et al. Distal rectus femoris surgery in children with cerebral palsy: Results of a Delphi consensus project. J Child Orthop. 2021;15(3):270-278.
- Rutz E, McCarthy J, Shore BJ, et al. Indications for gastrocsoleus lengthening in ambulatory children with cerebral palsy: a Delphi consensus study. J Child Orthop. 2020;14(5):405-414.
- Salazar-Torres JJ, Church C, Shields T, et al. Comparison of surgical outcomes for distal rectus femoris transfer and resection surgeries in children with cerebral palsy with stiff knee gait. J Pediatr Orthop. 2021;41(8):520-524.
- O’Brien DF, Park TS. A review of orthopedic surgeries after selective dorsal rhizotomy. Neurosurg Focus. 2006;21(2):e2.
- MacWilliams BA, McMulkin ML, Duffy EA, et al. Long-term effects of spasticity treatment, including selective dorsal rhizotomy, for individuals with cerebral palsy. Develop Med Child Neuro. 2022;64(5):561-568.
- Boyer ER, Duffy EA, Walt K, et al. Long-term functional outcomes after an external femoral derotation osteotomy in individuals with cerebral palsy. Gait & Posture. 2021;87:184-191.
- Stotts AK, Carroll KL, Naatz E, et al. Outcome of gastrocnemius soleus facial lengthening in ambulatory patients with cerebral palsy. J Pediatr Orthop. 2022;42(1):e65-e71.
- Sees JP, Maguire K, Prestowitz S, et al. Incidence of deep vein thrombosis in cerebral palsy following an orthopaedic surgical event. J Pediatr Orthop. 2022;42(5):285-288.