
Surgical/Technical Tips
Use of a “Fast, Feed, and Wrap” Technique with Local Anesthesia for In-Office Surgical Correction of Postaxial Polydactyly Type B in Infants
1Dell Medical School - The University of Texas at Austin, Central Texas Pediatric Orthopedics and Scoliosis Surgery, Austin, TX; 2Dell Children’s Trauma and Injury Research Center, Dell Children’s Medical Center, Austin, TX; 3Dell Medical School - The University of Texas at Austin, Institute of Reconstructive Plastic Surgery of Central Texas, Austin, TX
Correspondence: Niamh D. McMahon, MS, 1301 Barbara Jordan Blvd., #300, Austin, TX 78723. E-mail: [email protected]
Received: June 22, 2022; Accepted: June 26, 2022; Published: August 1, 2022
DOI: 10.55275/JPOSNA-2022-0074
Volume 4, Number 3, August 2022
Abstract:
Surgical correction of postaxial polydactyly Type B has several potential advantages over the traditional approach of suture ligation. Benefits include achieving more cosmetic results, reduced risk of neuroma or bothersome scar, and decreased likelihood of needing a second procedure. Previous reports with small numbers of patients have described surgical polydactyly excision using local anesthesia only, either in the operating room or office setting. We now routinely perform these removals in the office using local anesthesia combined with a fast, feed and wrap (FFW) technique to improve the comfort of the patient and parents. Details and photos of this technique are provided, and we encourage those who still perform routine suture ligation to consider this method as a simple and effective alternative.
Key Concepts:
- We have found that routine surgical excision of postaxial polydactyly Type B is superior to suture ligation for attaining more cosmetic results and avoiding future pain and discomfort.
- Removal is performed in-office using local anesthesia and a fast, feed and wrap (FFW) technique.
- Surgical excision using the technique described below has led to fewer complications and more functionality, in our experience.
Introduction
Postaxial polydactyly Type B involves the presence of a small, non-functioning supernumerary digit that is often pedunculated.1 Most common among African-American children in whom the condition usually follows an autosomal-dominant inheritance pattern, it can also be seen in children of any race or ethnicity.1,2 Suture ligation has been a common method of removing these digits and is performed using suture or vascular clip to tie off the digit, which then becomes necrotic and usually falls off.2 Families may be uncomfortable with the appearance of the digit until it falls off, and there are also risks of complications such as infection, a residual bump left on the ulnar border of the hand, and scarring. Some patients require a second procedure after suture ligation, either because of incomplete amputation of the digit or potentially painful neuroma formation.2–4 In fact, up to 40% of infants undergoing suture ligation experience a residual, tender bump.5 Figure 1 shows typical complications seen in our practice.
Figure 1. Typical complications seen in our practice after suture ligation. Necrosis (top) and residual bump after suture ligation (bottom).

Description of the Method
We established a procedure to routinely perform in-office surgical excision of postaxial Type B supernumerary digits with the parents holding the child, using a combination of local anesthetic and the natural infant behavior of postprandial sleep. Refer to Figure 2, below, for typical surgical set up. The fast, feed, and wrap (FFW) technique begins with the parents withholding feeding and napping 3-4 hours prior to the scheduled procedure. The patient and parents are brought into the exam room. Local anesthesia of the digit to be removed is obtained by injecting 1% lidocaine with epinephrine with a 27- or 30-gauge needle on a 1-cc syringe. Generally, about 0.5 cc total volume is injected in two sites—first just proximal to the base of the digit and then at the base. The inclusion of epinephrine helps with hemostasis. Of note, we do not use any topical anesthetic. We have not found it necessary, and a 2017 study concluded there was no strong evidence to support the effectiveness of topical anesthetic for procedures involving skin puncture in infants.6 We also do not use any type of tourniquet or cautery and have encountered no major issues with bleeding.
Figure 2. Supplies used to perform in-office excision (left). Supplies necessary include, but are not limited to, #15 blade, 2 x 2 gauze square, and self-adherent wrap. The area is draped with a sterile surgical towel with a hole cut in it to cover the rest of the arm and infant (right).
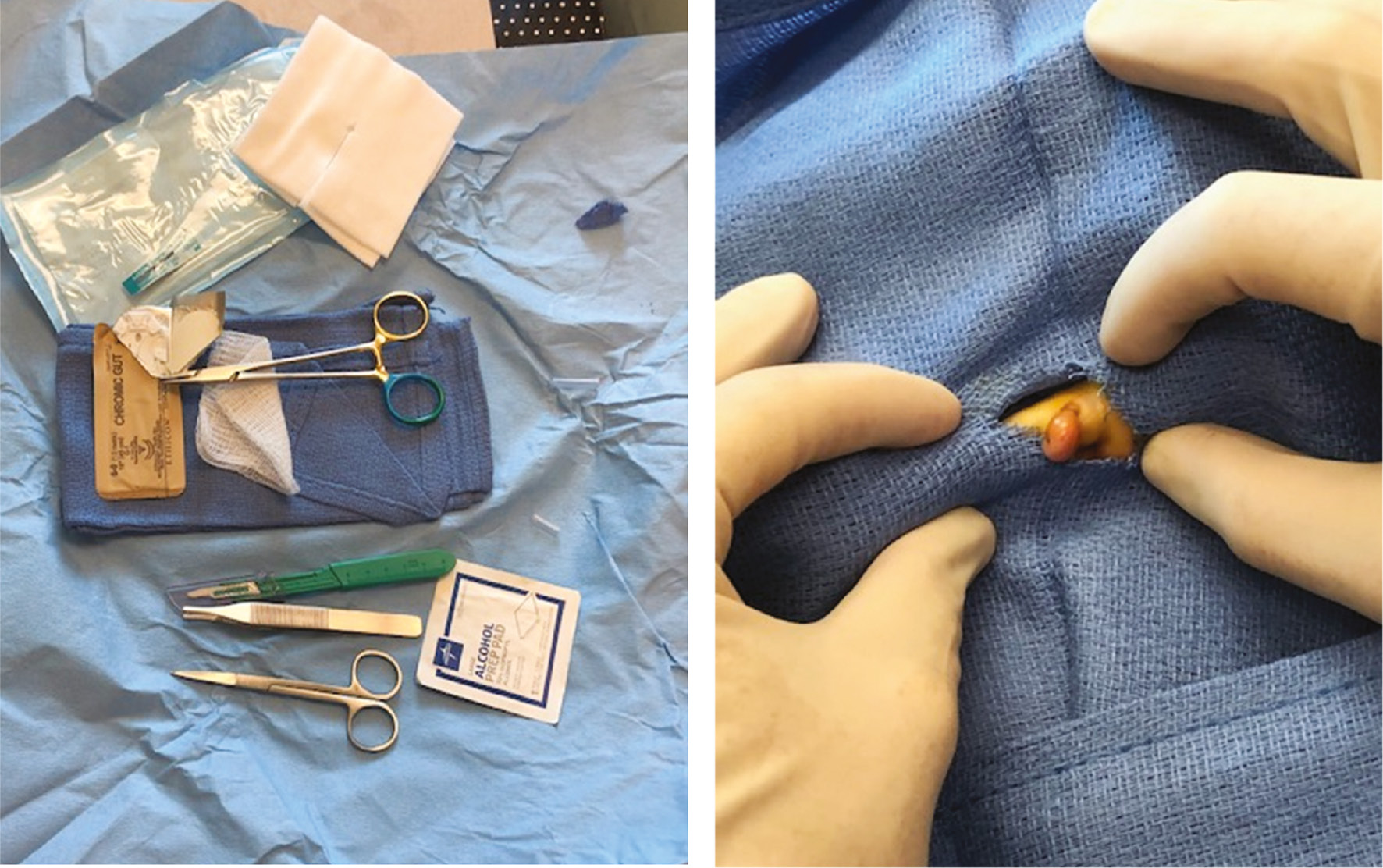
After administration of local anesthetic, the parent is instructed to feed the child, during which time the clinician is free to leave the room. In our experience, most patients will fall asleep 15–20 minutes after the injection, after being fed.
The infant is then wrapped or swaddled and held on a parent’s lap, using pillows and blankets for support as needed. An assistant holds the baby’s hand for the procedure. The area is draped with a sterile fenestrated towel and prepped using Chloraprep or betadine, depending on the surgeon’s preference.
An elliptical incision is made using a disposable #15 blade, or the stalk is amputated with iris scissors. The skin is closed with a 6-0 chromic suture. Care is taken to make sure the digital nerve to the supernumerary digit is not entrapped in the skin closure. A small bandage is applied using a 2 x 2 gauze square and self-adherent wrap. The dressing can be removed at home in 2 days. At that time, parents are instructed to gently wash with soap and water and apply a Band-Aid for 7 days. Patients can be followed up in 2 weeks if needed, though this is rarely the case in our practice.
Comparison to Other Methods
Given that ulnar polydactyly is one of the most common congenital anomalies of the upper extremities,2 there is a surprising dearth of rigorous studies in the medical literature comparing outcomes and patient and parent satisfaction with available treatment methods.3 We would argue that routine surgical excision is superior to suture ligation for attaining more cosmetic results and avoiding future pain and discomfort. However, we suspect that suture ligation remains commonly used because it is fast, simple, avoids general anesthesia, and many clinicians are not comfortable with performing surgical excision using local anesthetic. We would argue that routine surgical excision is superior to suture ligation for attaining more cosmetic results, as seen in Figure 3, and avoiding future pain and discomfort.
Figure 3. Post-excision results.

There are multiple valid reasons for avoiding unnecessary general anesthesia among infants, including safety and possible long-term risk of developmental delays, learning disabilities, and attention-deficit hyperactivity disorder.7 In theory, performing a painful procedure in an awake infant may also affect the child’s processing and experience of pain into adulthood.8 Distress of the parent or caregiver is also a concern with any potentially painful procedure in an infant. However, local anesthetic can be used safely and effectively for minor procedures in infants. In fact, a 2021 report of 51 infants undergoing surgical excision for postaxial polydactyly Type B under local anesthesia in the operating suite showed excellent results and overall positive parent satisfaction with the procedure.5 One of the biggest benefits of surgical excision is that it allows retraction of the accessory digital nerve, thereby preventing later residual pain.5 A small study of 30 children from 2016 reported success with in-office surgical resection using local anesthesia. In this cohort, parents reported no symptoms of neuroma or pain at the site on follow-up.9 Though it was unclear how long the children were followed, it is logical that the risk of a painful residual bump would be much lower with surgical excision.
Variations of this strategy have been described under names such as feed and sleep, feed and swaddle, feed and wrap, or fast, feed and wrap (FFW). Most of the publications assessing the utility of this anesthetic strategy have involved imaging, particularly for MRI of infants.6,10–12 Imaging procedures require the infant to be still but do not generally involve any painful stimulus. However, one study showed successful use of a “fast, feed and wrap” technique along with local anesthesia for peripherally inserted central catheter (PICC) placement.13 The findings of this study are intriguing as they suggest this technique may be useful in a variety of other clinical situations outside of imaging. This aligns with our positive experiences performing in-clinic correction of postaxial polydactyly Type B using a combination of fast, feed and wrap (FFW) technique and local anesthetic.
Summary
Our experience in doing this for more than 9 years has been very positive. This is consistent with what has been reported in the literature. No procedure is free of complications; however, this technique is expected to have a low rate of complications. These may include superficial infection or reaction to the chromic suture.
We allow the incision to get wet with clean soapy water at day 2. Some parents are anxious and refuse to get the incision wet, leading to retention of the sutures longer than expected. In this rare case, we removed the suture in clinic. We counsel families that there will be a scar. The senior authors (HPG and SLH) have yet to see any hypertrophic scars or keloids from this procedure.
In our experience over the last 13 years using this combination of local anesthetic and a fast, feed, and wrap (FFW) technique, surgical correction of postaxial polydactyly Type B can be safely and easily performed in the medical office setting. While a larger study to compare this technique to other methods such as suture ligation might be ideal, we wonder whether it is truly necessary considering the obvious advantages of surgical excision, the ease with which in-office excision has become our established practice, and the opportunity to achieve a more cosmetic and functional result.
Disclaimer
The authors have no conflicts of interest to disclose.
References
- Hiro ME, Gottschalk HP, Light TR. Ulnar polydactyly and Ulnar dimelia. In: Laub Jr DR, ed. Congenital Anomalies of the Upper Extremity: Etiology and Management. Cham: Springer International Publishing; 2021:351–366.
- Abzug JMMD, Kozin SHMD. Treatment of postaxial polydactyly type B. J Hand Surg Am. 2013;38(6):1223-1225.
- Chopan M, Sayadi L, Chim H, et al. To Tie or Not to Tie: a systematic review of postaxial polydactyly and outcomes of suture ligation versus surgical excision. Hand. 2020;15(3):303-310.
- Grenier G, Samora JB. Resection of postaxial supernumerary digits. Cham: Springer International Publishing; 2019:409-416.
- Bjorklund KA, O’Brien M. Local anesthesia alone for postaxial polydactyly surgery in infants. Hand (N Y). 2021:1558944721994255-1558944721994255.
- Foster JP, Taylor C, Spence K. Topical anesthesia for needle-related pain in newborn infants. Cochrane Database Syst Rev. 2017;2(2):Cd010331.
- Antonov NK, Ruzal-Shapiro CB, Morel KD, et al. Feed and wrap MRI technique in infants. Clin Pediatr. 2017;56(12):1095-1103.
- Schwaller F, Fitzgerald M. The consequences of pain in early life: injury-induced plasticity in developing pain pathways. Eur J Neurosci. 2014;39(3):344-352.
- Carpenter CL, Cuellar TA, Friel MT. Office-based post–axial polydactyly excision in neonates, infants, and children. Plast Reconstr Surg. 2016;137(2):564-568.
- Shariat M, Mertens L, Seed M, et al. Utility of feed-and-sleep cardiovascular magnetic resonance in young infants with complex cardiovascular disease. Pediatr Cardiol. 2014;36(4):809-812.
- Templeton LB, Norton MJ, Goenaga-Díaz EJ, et al. Experience with a “Feed and Swaddle” program in infants up to six months of age. Acta Anaesthesiol Scand. 2020;64(1):63-68.
- Weng W, Reid A, Thompson A, et al. Evaluating the success of a newly introduced Feed and Wrap protocol in magnetic resonance imaging scanning of the temporal bone for the evaluation of congenital sensorineural hearing loss. Int J Pediatr Otorhinolaryngol. 2020;132:109910-109910.
- Laing S, Burgoyne LL, Muncaster M, et al. Infant peripherally inserted central catheter insertion without general anesthesia. Pediatr Anesth. 2020;30(11):1211-1215.