
Current Concept Review
Pediatric and Adolescent Jehovah’s Witnesses: Considerations for Safe and Ethical Orthopaedic Procedures
1Department of Orthopaedics, Baylor University Medical Center, Dallas, TX; 2Department of Orthopaedics, School of Medicine, Case Western Reserve University, Cleveland, OH; 3Department of Orthopaedic Surgery, Renown Pediatric Orthopedics and Scoliosis, Reno, NV
Correspondence: Cynthis Wong, MD, Baylor University Medical Center, Department of Orthopaedics, 3500 Gaston Ave., 6th floor Hoblitzelle, Dallas, TX 75246. E-mail: [email protected]
Received: June 28, 2022; Accepted: June 6, 2022; Published: August 1, 2022
DOI: 10.55275/JPOSNA-2022-0086
Volume 4, Number 3, August 2022
Abstract:
Jehovah’s Witnesses are members of a restorationist Christian denomination widely known for their refusal of blood transfusions. Most important for consideration of the pediatric orthopaedic surgeon, are patients undergoing high-risk cases such as spine and pelvic surgery. While previous case rulings have been quite clear in outlining the treatment of young children of Jehovah’s Witnesses, there is much more variability in the treatment of those who are adolescents and who may have the capacity to consent. In order to provide the best possible care and avoidance of harm, we present legal, ethical, and medical issues surrounding treatment of Jehovah’s Witnesses. Preoperative planning requires frequent communication with family, multi-disciplinary coordination, verification of acceptable blood products, and anemia optimization. By utilizing various intraoperative and postoperative techniques, safe surgery can be successfully performed with similar outcomes as other patient groups.
Key Concepts:
- Jehovah’s Witnesses are a restorationist Christian denomination who are notable in the medical community for their refusal of blood transfusions.
- In treating pediatric Jehovah’s Witnesses, conversations should ensure the decision-making capacity of the patient or parent, that the patient is free from coercion, and that they are able to convey understanding.
- Preoperative planning requires multi-disciplinary coordination, verification of acceptable blood products, and anemia optimization.
- By utilizing various intraoperative and postoperative techniques, safe surgery can be successfully performed with similar outcomes as other patient groups.
Introduction
Jehovah’s Witnesses are members of a restorationist Christian denomination widely known for their refusal of blood transfusions, which is critically important in consideration for large blood loss cases such as spine and pelvic surgery.1 It is important to examine the legal, ethical, and medical issues surrounding the treatment of Jehovah’s Witnesses in order to have collaborative conversations towards the best possible care and avoidance of harm. The rights of children and adolescents to refuse treatment must also be understood. In the following, we aim to provide background information, elucidate legal and ethical considerations for pediatric patients, and describe perioperative techniques in performing bloodless surgery.
Background
The Jehovah’s Witness denomination was founded in the 1870s with beliefs centered on the acceptance of the Bible and in some circumstances, literal interpretation of the text. Worldwide, there are over 8.7 million Jehovah’s Witnesses, with just over 1.2 million residing in the United States.2 More can be learned about the denomination from their website: https://bit.ly/3yArEdh.
Subscribers to the Jehovah’s Witness religion refuse blood products based off of several passages from the Bible that forbid the ingestion of blood (Genesis 9:4; Leviticus 17:10; Deuteronomy 12:23; Acts 15:28, 29).3,4 The governing body of Jehovah’s Witnesses, The Watchtower Society states that based upon parallels made with parenteral nutrition, receiving blood transfusions is considered the same as eating blood.5 Ingestion of blood may result in a type of excommunication for members and the loss of eternal life. However, The Watchtower Society elaborates, stating that those that have received blood products are not immediately disfellowshipped, and instead, patients who had transfusions under duress would have “kindness … shown and pastoral help offered.”6 Regardless, the refusal of blood products is a core tenet of their faith. Forced transfusions can cause irreparable psychological harm.6
Ethical and Legal Principles of Medicine: Application to Children and Adolescents
When evaluating care for young Jehovah’s Witnesses, it is useful to consider the four principles of medical ethics as stated by Beauchamp and Childress: autonomy, beneficence, non-maleficence, and justice.7 Practicing autonomy necessitates liberty (the ability to make a choice free from controlling influences) and agency (the capacity to act intentionally). Beneficence refers to actions done to benefit others, while non-maleficence refers to avoiding actions that harm others. Finally, justice refers to the fair allocation of resources.
In the U.S., patient autonomy is heavily weighted against other principles when applied to adults with decision-making capacity.8 The ethics and legality of medically necessary interventions in young children have also been established. Courts have consistently deemed that the state can intervene to protect children and that parents “do not have an absolute right” to medical treatment refusal.9 Furthermore, courts have also allowed physicians to provide emergency medical care to minors without consent of their parents.10 This should not mean that the issue is solved for surgeons caring for young patients. For example, if there is no immediate risk to the child, the courts will often support the parental decision.11
Adolescents present a particular challenge, as their evolving maturity may allow for capacity for decision-making and thus, autonomy. Legislation regarding this matter is inconsistent and state dependent, so these cases must be evaluated individually. At the time of writing, 17 states have a mature minor doctrine or provisions which allow some minors to consent to medical treatment without parental consent (Table 1).9,12 Others states declare adolescent Jehovah’s Witnesses immature and lacking in ability to understand, deferring medical decisions to their parents or the courts.
Table 1. States Which Allow Some Form of Adolescent Consent
| States | ||
|---|---|---|
| Alabama | Kansas | Oregon |
| Alaska | Louisiana | Pennsylvania |
| Arkansas | Maine | South Carolina |
| Delaware | Massachusetts | Tennessee |
| Idaho | Montana | West Virginia |
| Illinois | Nevada | |
It is worth noting however, that capacity to consent to treatment is not the same as capacity to refuse treatment. Multiple cases have emerged in which adolescents were not given the right to refuse treatment, instead becoming wards of the state, secondary to the severe consequence of their refusal.13 This was seen in the case of Daniel Hauser, a 13-year-old in which the court did not allow him to refuse chemotherapy on his religious grounds.14 In the case of Shannon Nixon, an adolescent with uncontrolled diabetes who had refused treatment, the Pennsylvania Supreme Court suggested that, while minors may consent to certain medical treatments, stricter evaluation should be held in refusals of care in life or death situations.14 Furthermore, in emergency situations, it is often difficult to assess the capacity of the adolescent. The state’s interest in preserving life often outweighs the parents’ and adolescent’s convictions.15 It is therefore reasonable to presumptively treat the minor in life-preserving situations if blood products cannot be avoided.
Approach to Children and Adolescents of Jehovah’s Witnesses
Conversations between physicians and parents (and/or adolescents) who refuse treatment are often difficult because physicians must balance several potentially conflicting principles of medical ethics. When treating children, decision-making authority is usually given to the parents. But adding further complexity, adolescents may have decision-making capacity and their wishes and decision may differ from their parents.
While these discussions are complex, the surgeon should first seek an understanding of the reasoning behind the refusal of treatment. Acknowledgement is critical in demonstrating the physician’s understanding of the patient’s values and their significance. This can also aid in forming a bridge of communication for future management. Conversations should ensure that the patient or parent is free of coercion, has decision-making capacity, and is able to convey understanding, ensuring that their refusal is not due to a misunderstanding. These conversations should be had privately, without members of the church, to ensure the patients’ choices can be freely expressed.
Preoperative discussions should include verification of acceptable treatments, accurate documentation, and coordination of multidisciplinary planning.16 It should be known what blood products the patient is willing to accept. For optimal surgical planning, the anesthesiologist, hematologist, and the rest of the peri-operative team should also be informed. The Watchtower Society provides a liaison that can be consulted for alternatives to blood transfusion in medical management if needed. Preoperatively, it is best that the family understands that the team will do all that they can to mitigate blood loss in keeping with their religious beliefs (e.g., do they consent to auto transfusion or not?). Yet by consenting to the procedure, they understand that their surgeons and the hospital are duty bound to transfuse blood if a critical anemia is reached. Consenting to the operation implies this concept and consultation with the hospital ethics committee as well as court resolution of the decision would be pursued. In this case, the court’s responsibility is to decide whether the choice of nonblood management will adequately meet the child’s needs. The hospital ethics committee and court consultation play a critical role in providing proper patient care as well as protecting the physician and hospital from potential liability.
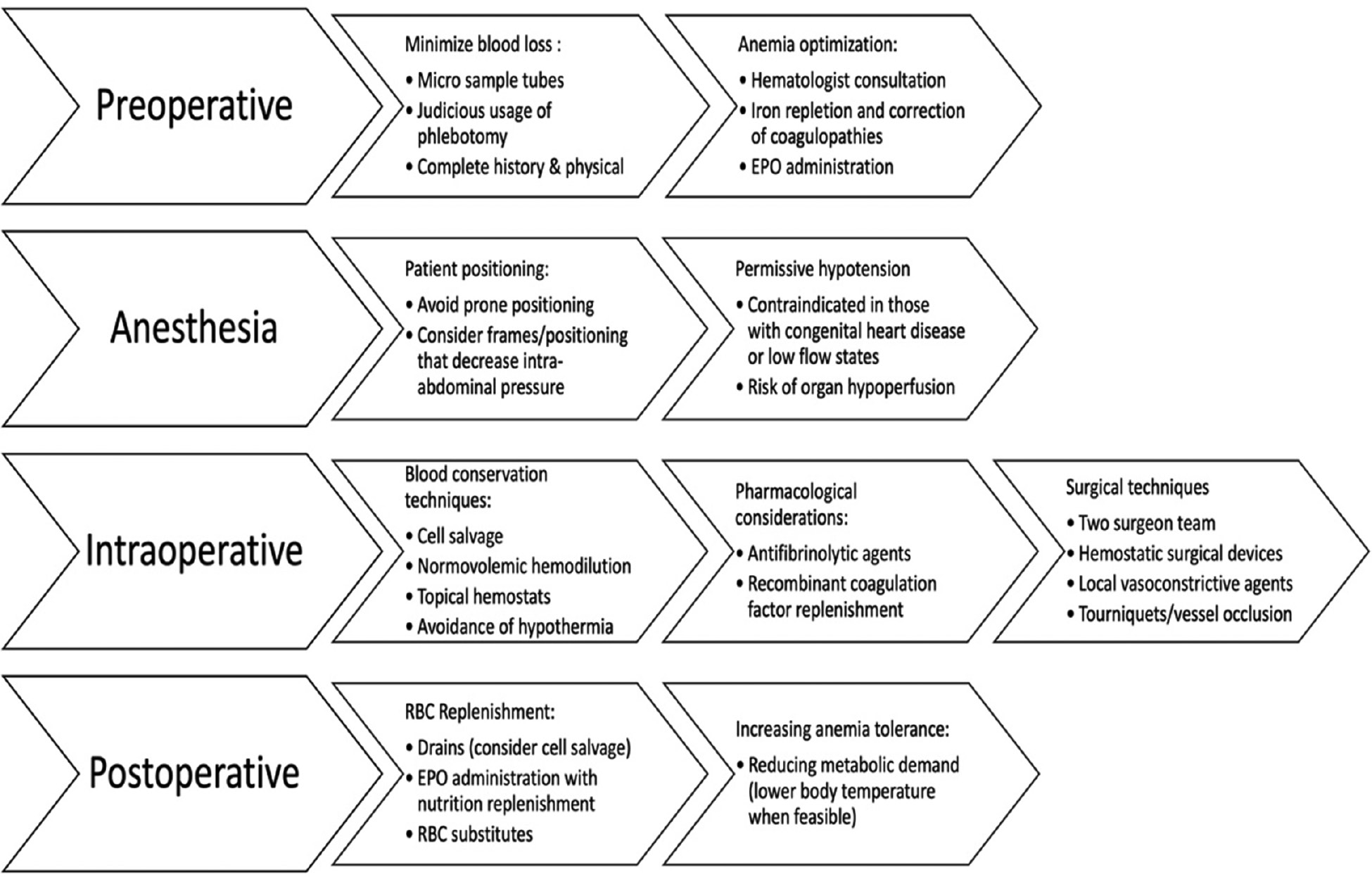
Perioperative Medical Management of the Young Jehovah’s Witness (Figure 1)
Figure 1. Brief outline of preoperative, anesthesia, intraoperative, and postoperative techniques for blood loss reduction.
Are All Blood Products Viewed Equally?
Jehovah’s Witnesses do not accept whole blood as well as major components of blood such as red blood cells, white blood cells, platelets, plasma, or hemoglobin. In addition, auto-transfusions of their own blood may not be accepted as some believe that blood removed from the body should be disposed of.17 However, blood substitutes with a minor blood derivative such as albumin, immune globulins, or clotting factors may be acceptable. Cell salvage may be used as long as the blood is maintained with the body in one continuous circuit. Completely synthetic blood substitutes are also acceptable in addition to fluids or heart lung machines (Table 2).
Table 2. Religiously Acceptable Strategies to Manage Blood Loss
| Acceptable | May be considered | Unacceptable |
|---|---|---|
|
|
|
Preoperative Considerations
Patients should be assessed to determine if they are at an increased risk of bleeding. If indicated, a preoperative consultation with a hematologist should address correction of any coagulopathies and anemia. Particularly, it is important to stop any medication that impairs clotting, correct coagulopathies, and correct anemia with iron supplementation preoperatively. Phlebotomy can be limited through the use of pediatric or micro sample tubes for laboratory draws. Potential vectors of blood loss such as menstruation or gastrointestinal ulcers must also be considered. Lastly, preoperative arteriograms can provide critical information regarding the vascular anatomy surrounding the target area. It may be possible to perform selective arterial embolization. This method has been shown to be useful in tumors and pelvic fracture surgeries.18
Preoperative exogeneous erythropoietin (EPO) has been shown to minimize transfusion requirements for surgical procedures with up to 20% total blood volume loss.19 Formulations without albumin are available and can be used for Jehovah’s Witnesses. Simultaneous iron, vitamin B12, and folate supplementation is required during treatment due to functional deficiencies caused by increased hematopoiesis. Adverse side effects include an increased risk of thromboembolism secondary to increased vascular resistance, arterial blood pressure, and decreased cardiac output.20 However, the associated improvement in oxygen carrying capacity typically outweighs these risks in anemic patients.21,22
Vitamin K and prothrombin complex concentrates are successful in the reversal of oral anticoagulants and reduction of blood product administration.23 These are plasma-derived agents; however, there is a formulation without human albumin and may be more amenable for some Jehovah’s Witnesses.
Pre-Incision Preparation
While some studies have shown that use of central neuraxial anesthesia may result in decreased blood loss,24–26 more recent studies have shown no significant difference between this approach and general anesthesia.27,28 As such, the operative team should employ their standard approach to anesthesia for the anticipated procedure.
Antifibrinolytic Agents. Antifibrinolytic agents such as tranexamic acid (TXA) or -aminocaproic acid (Amicar) have been shown to reduce blood transfusion needs by up to 69% in orthopaedic procedures such as joint arthroplasty and fracture open reduction and internal fixation.29–34 There was no increased risk of total thromboembolic events. TXA was found to be 6-10 times more potent than -aminocaproic acid;35 however, the only FDA-approved usage for tranexamic acid is short-term for patients with hemophilia and menorrhagia.36 Topical and intravenous formulations are available, with the suggested route of administration and amount is highly variable depending on the patient’s needs. One meta-analysis demonstrated improved blood loss reduction with high dosage of TXA (defined as a bolus of 10 to 100 mg/kg with a maintenance dose greater than 10 mg/kg/h) when compared to a low dosage in adult spinal surgery.37 Dosage of 100 mg/kg with a maintenance rate of 10 mg/kg/h has previously been successfully utilized in pediatric spine surgery.38
Recombinant Coagulation Factors. Recombinant Factor VII, VIII, and IX concentrates are also available. Factor VIII and IX concentrate administration has been successfully utilized in conjunction with other factors in improving clot formation, platelet activation and prevention of excess bleeding,39,40 Unlike cryoprecipitate or fresh frozen plasma, these are produced without human blood and are thus acceptable to most Jehovah’s Witnesses. Recombinant factor VIIa has also been used intraoperatively to reduce mean blood loss, in obstetric patients with dilutional coagulopathy, or postoperatively in open heart surgery.41–43 However, its value in orthopaedic surgery is unproven. Two randomized controlled trials for traumatic pelvic fractures and major spinal surgery demonstrated no significant difference between surgical blood loss and transfusion volume.44 Guidelines from the European Society of Anaesthesiology thus limit the use of recombinant factor VIIa for refractory bleeding that cannot be stopped by other conventional methods.45
Recombinant fibrinogen can also be utilized. A recent meta-analysis on the effectiveness of fibrinogen on blood loss was unable to draw any conclusions due to the limited number of studies.46 However, some studies have shown effectiveness as prophylaxis for hemorrhage or correction of dilutional coagulopathy.47–49 During hemorrhage, fibrinogen depletion is thought to occur first among other coagulation factors. Low preoperative levels have been linked to increased blood loss in orthopaedic surgery.48,50,51 Administration of crystalloids and colloids has also been found to interfere with fibrinogen and fibrin polymerization.48 This can be reversed with administration of fibrinogen concentrate intraoperatively. Thus, in the setting of dilutional coagulopathy, prophylactic recombinant fibrinogen administration can also be considered.
Desmopressin. Desmopressin stimulates the release of von Willebrand factor and factor VIII and can correct coagulopathies in hemophilia A. Investigations for desmopressin usage intraoperatively have demonstrated variable results. Multiple Jehovah’s Witness cases have shown increased hemostasis with desmopressin administration.52 In orthopaedics, Kobrinsky, et al. successfully demonstrated the reduction of blood loss by 32.5% in spinal fusion surgery through desmopressin administration.53 Conversely, a recent Cochrane review of 65 trials demonstrated that desmopressin administration has little to no impact on transfusion probability or all-cause mortality.54 Given this, Beholz et al. suggest a preoperative test dosage to assess the patient response to desmopressin prior to intraoperative administration.52 European guidelines recommend desmopressin in trauma patients for those on antiplatelet agents or those with acquired platelet dysfunction.55
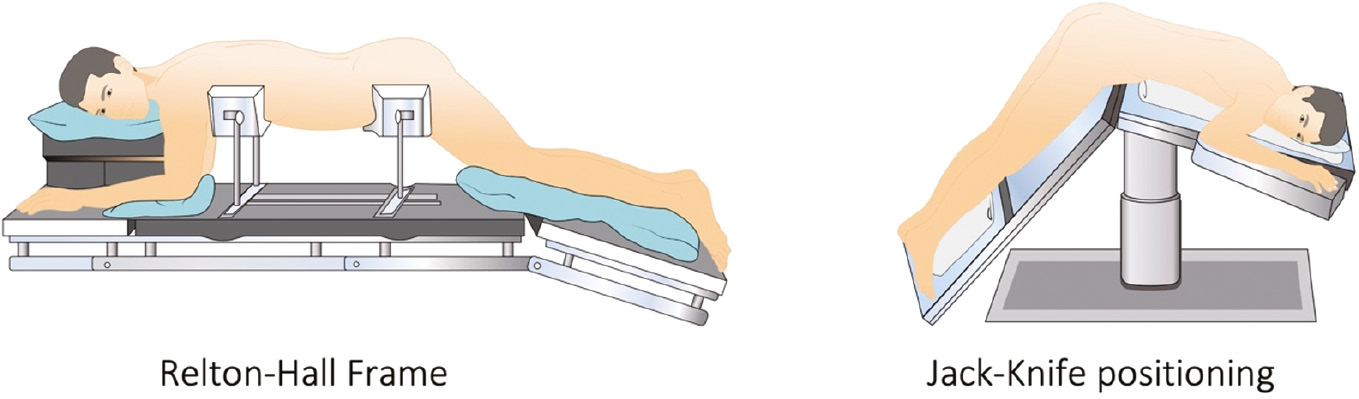
Patient Positioning. Patient positioning has been shown to be a simple and effective method of reducing intraoperative blood loss. For example, the prone position, particularly in spine surgery, is noted to cause compression of the inferior vena cava and increased intra-abdominal and intra-thoracic pressure. This results in decreased venous return, cardiac index, and stroke volume. The increased hydrostatic pressure and vessel engorgement leads to increased bleeding at the surgical site.56,57 Increased intra-abdominal pressure can also increase bleeding from vertebral veins during spinal surgery, potentially prolonging surgical time.58 Interventions such as utilizing wide pads, a Jackson table, or applying chest rolls may help decrease intra-abdominal pressure and resulting blood loss.59 A Relton-Hall or Prone Jackson frame also allows the abdominal viscera to hang freely, leading to decreased IVC pressure (Figure 2).60,61 Jack knife positioning has been shown to decrease intra-abdominal pressure and venous bleeding in spinal surgeries.62
Figure 2. Relton-Hall frame and Jack-Knife positioning to decrease blood loss.
Depending on the procedure, other positions have been demonstrated to decrease blood loss. For supine patients, tilting the patient slightly to the left may reduce inferior vena cava compression. Elevating the site of surgery to a level above the heart, when possible, may also reducing bleeding by decreasing venous pressures.
Avoidance of Intraoperative Hypothermia. Hypothermia can increase the amount of blood loss by as much as 16% as well as the risk of wound infection, cardiovascular events, and prolonged recovery time.63 Hypothermia can also cause platelet dysfunction, with even mild perioperative hypothermia associated with increased blood loss and risk of transfusion.64
Hypotensive Anesthesia. Permissive hypotension is a well-documented practice that consists of maintaining mean arterial pressure between 50-65 mm Hg. Multiple studies have demonstrated that this strategy reduces blood loss in patients undergoing orthopaedic surgery and reduces transfusion requirements by as much as 40%.18,65,66 Specifically, effectiveness in scoliosis surgeries has been well-documented, decreasing blood loss as much as 55% and shortening operative time.67,68 While no studies to our knowledge have examined the risks of permissive hypotension, there is a theoretical risk of organ hypoperfusion. Therefore, those with congenital heart disease or signs of low flow states are contraindicated from receiving permissive hypotension. When performing idiopathic spinal deformity surgery, hypotension during surgical approach and implant placement is widely accepted, yet mean arterial blood pressure should be raised when corrective spine manipulations are taken. It may be wise to have higher blood pressures when spinal surgery is more complex or when treating congenital spine deformity.
Autotransfusion. Normovolemic hemodilution consists of the removal of whole blood prior to surgery with simultaneous volume replacement with crystalloid or colloid solutions to a hematocrit of 20-30%. This would dilute the total blood lost during surgery. The blood is then reinfused back into the patient as needed or during closure of the wound. This technique has been well demonstrated in a variety of surgeries including total knee and hip replacements to reduce blood transfusion requirements.69,70
Intraoperative Strategies
Red Blood Cell Salvage. Intraoperative cell salvage is a safe and cost-effective alternative to blood transfusion, reducing the need for transfusion across a variety of surgical specialties.16,39,71,72 Guidelines recommend cell salvage when expected operative blood loss is greater than 500 mL, the amount required for a clinically relevant amount of blood to be reinfused.73 This technique involves collecting blood that is lost during surgery or through wound drains and reinfusing it after centrifugation, washing, and anticoagulation. While many Jehovah’s Witnesses will require the blood to remain in one continuous circuit within their body, some may also accept cell salvage from drains.
Contraindications to cell salvage are debated and risks of cell salvage must be weighed against its benefits. Traditionally, infection, malignancy, and sickle cell disease were relevant contraindications to cell salvage due to concerns for bacteremia, seeding of malignancy and inducing sickling.63,74 However, a study by Waters et al. demonstrated a 99% reduction in bacterial contamination with proper cell washing and leukocyte depletion filtration.75 It is unclear what effect the remaining bacteria may have. Further evidence suggests this technique can also be successfully used to remove tumor cells.74,76 Regarding sickle cell disease, two case reports have demonstrated successful usage during hip arthroplasty and posterior spinal fusion and instrumentation for scoliosis, in which 15-20% of the cells found to be sickled.77,78 Another study reported 50% of cells in a blood sample from a patient with sickle cell disease were sickled prior to transfusion.79 The Association of Anaesthetists of Great Britain and Ireland therefore suggest a blood film to be utilized prior to reinfusion in order to assess for sickling, and that the decision to use this technique should be discussed individually with each patient.80
Topical Hemostatic Agents. Both passive and active topical hemostatic agents exist (Table 3). Passive hemostats, such as cellulose and gelatin, work by promoting platelet activation and producing a matrix at the site of bleeding. They are suitable for patients with an intact coagulation system and are excellent for reducing incisional oozing of blood.81 In coagulopathies, active hemostats such as fibrin sealants can be utilized. Active hemostats are derived from human fibrinogen, have biological activity, and are designed to mimic the last step of coagulation. However, results have been variable, with increased hemostasis in patients undergoing total knee arthroplasty but not in total hip arthroplasty.82 Further investigation is required before effectivity of fibrin sealants can be determined. Furthermore, as they are derived from human fibrinogen, some Jehovah’s Witnesses may not be amenable to their use.83
Table 3. Active and Passive Hemostatic Agents
| Active agents | Mechanism of Action |
| Thrombin, thrombin + gelatin, thrombin + collagen | Converts fibrinogen into fibrin and also stimulates platelet aggregation |
| Fibrin sealant | Fibrinogen gets transformed into fibrin through the addition of thrombin and factor XIII, mimicking the final step of the coagulation cascade |
| Passive agents | Mechanism of Action |
| Collagen | Attracts platelets which adhere to large fibrils, initiating platelet aggregation |
| Cellulose | Acts similarly to gauze in hemostasis, serving as a bioabsorbable network |
| Gelatin | Mechanical tamponade effect by swelling of gelatin. |
| Polysaccharides | Dehydrates blood, concentrating the solid components in order to increase formation of a barrier for the bleeding |
| Bovine albumin and glutaraldehyde | Binds to proteins of bleeding creating mechanical seal |
| Polyethylene glycol polymers | Absorbs fluids and expands, decreasing bleeding |
| Cyanoacrylate adhesive | Polymerizes in contact with organic proteins, forming a hardened shell on surface |
Surgical Considerations. Operative technique may be the single most important factor in blood loss.84 Operative times directly correlate with blood loss in multiple surgeries, including total joint arthroplasty and posterior spinal fusion.84,85 It is therefore important that the surgeon with the greatest expertise performs the procedure. Other possibilities to consider are staged approaches, a dual attending surgery (with the goal of reduced duration of surgery), and use of surgical tools such as tourniquets, electrocautery, argon-beam coagulation, topical hemostatic agents, ultrasonic bone scalpels, and local vasoconstrictive agents86,87 During peak blood loss, packing sponges soaked in adrenaline can be utilized.88 Temporary aortic or intra-iliac balloon occlusions have also been demonstrated to decrease blood loss in sacral tumor resection, acetabulum fracture, joint, and hip arthroplasty.89–92 However, this has associated risks of thrombus formation, balloon rupture, or hemodynamic ischemia. Lastly, usage of tourniquets for the purpose of reducing blood loss is controversial, with multiple meta-analyses demonstrating no difference in overall blood loss.93,94 Some studies even suggest that TXA alone is superior to the use of tourniquet.95 Despite this, tourniquets may still be advantageous for improving surgical field of vision.
Postoperative Techniques
Drains. Closed suction drainage is frequently used postoperatively in orthopaedic surgery but is associated with an increased risk of blood transfusions.96 This may be combated with reinfusion of blood from the wound drain (if permitted) but requires timely intervention and reinfusion within 6 hours.97
Increasing Synthesis of Red Blood Cells. Postoperative EPO administration in conjunction with IV iron, vitamin B12, and folate is highly effective in recovery of anemia in Jehovah’s Witnesses.39,98 While there is no defined dosage of erythropoietin for this situation, high doses at 600 μg/kg daily for 7 days or 600 μg/kg every other day have been demonstrated to be effective. Recently developed biomathematical models for predicting hemoglobin changes with iron and EPO supplementation can also be used to predict nutrition requirements and response.99
Red Blood Cell Substitutes. Two main classes of red blood cell substitutes exist but have been found to have significant safety concerns.21,100,101 To our knowledge, no trials have been performed in pediatric populations; therefore, we cannot recommend use of these products at this time.
Reducing Metabolic Demand. A few case reports have demonstrated the usage of deliberate hypothermia in Jehovah’s Witness patients, which reduces metabolic demand in critically ill patients by reducing tissue oxygen requirements.101–103 By lowering the body temperature to 30-32 degrees C, total oxygen consumption drops by approximately 48%. Neuromuscular blockade can similarly be used to reduce oxygen utilization. However, benefits of the therapy must be outweighed against the risks, which include cardiac arrhythmias and an association with increased blood loss perioperatively.104,105
Red Blood Cell Replenishment
While the goal is to avoid non-autologous transfusion, it is important to understand when transfusions are indicated. In patients who are not critically ill, there has been demonstrated tolerance of a hemoglobin around 7 g/dL.106 The threshold for anemia tolerance is not known, however. An interventional study by Weiskopf et al. showed adequate oxygenation to tissues in hemoglobin levels as low as 5 g/dL in healthy individuals.107 Experiences with Jehovah’s Witnesses have shown reported survival in cases with postoperative hemoglobin as low as 1.4 g/dL.108 However, this finding should be tempered by another study demonstrating a 2.5 times increase in risk of cardiac side effects with each 1 g/dL reduction in Hb below 8 g/dL.109 Levels below 4–5 g/dL were associated with a 34.4% mortality and 57.7% rate of side effects.109 It is therefore important to keep these thresholds in mind when evaluating actual replenishment needs. Acceptable blood loss can easily be calculated preoperatively with patient weight, patient starting hemoglobin, and tolerable post-operative hemoglobin (Table 4).
Table 4. Allowable Blood Loss Calculation (if estimated to be 50% TBV)
| Total Blood Volume (TBV) | Allowable Blood Loss (ABL) | |
|---|---|---|
| Children & male adults | 75 mL/kg | Weight (kg) × (TBV) × 0.5 |
| Adolescent male | 70 mL/kg | Weight (kg) × (TBV) × 0.5 |
| Adolescent & adult females | 65 mL/kg | Weight (kg) × (TBV) × 0.5 |
Summary
Pediatric orthopaedic Jehovah’s Witness patients provide significant ethical challenges. Physicians must be knowledgeable and respectful of the patient and family’s beliefs while doing no harm. We have outlined the ethical and legal issues surrounding care for adolescents and an approach to conversations with patients as well as aimed to provide preoperative, intraoperative, and postoperative strategies for maintaining hemostasis, minimizing blood loss, and increasing anemia tolerance. For high-blood loss cases such as tumor resection, spine and pelvic surgery, multiple osteotomies, and small allowable blood loss cases in young children, we recommend a team approach. Particularly in the case of elective surgery, this may include involvement of not only the orthopaedic surgeon, but also a co-surgeon, anesthesiologist, hematologist, and the hospital ethics committee.
Proper understanding and implementation of the above techniques has allowed complex care of Jehovah’s Witness patients without transfusion with comparable results as patients who have had transfusion.110 Risk of death and outcomes for Jehovah’s Witnesses after major trauma is now similar when compared to patients amongst other religious groups.111 In orthopaedic surgery, these techniques have been used in pediatric Jehovah’s Witnesses undergoing spinal deformity surgeries without any intraoperative complications.112 With the use of frequent communication with families, multidisciplinary preoperative planning, and blood conservation techniques, major orthopaedic surgeries can be completed successfully in pediatric Jehovah’s Witnesses while respecting their beliefs.
Disclaimer
No funding was received. The authors have no conflicts of interest to disclose pertaining to this manuscript.
Additional Links
- American Academy of Orthopaedic Surgeons (AAOS) Guidelines for Intraoperative Bleeding—https://bit.ly/3RrNYhU
- About Jehovah’s Witnesses—https://bit.ly/3yArEdh
References
- Ialenti MN, Lonner BS, Verma K, et al. Predicting operative blood loss during spinal fusion for adolescent idiopathic scoliosis. J Pediatr Orthop. 2013;33(4):372-376.
- 2020 Grand Totals. Available at: https://www.jw.org/en/library/books/2020-service-year-report/2020-grand-totals/.
- Why Don’t Jehovah’s Witnesses Accept Blood Transfusions? [cited 2021 April 5th]; Available at: https://www.jw.org/en/jehovahs-witnesses/faq/jehovahs-witnesses-why-no-blood-transfusions/.
- What Does the Bible Say About Blood Transfusions? [cited 2021 April 5th]; Available at: https://www.jw.org/en/bible-teachings/questions/bible-about-blood-transfusion/.
- Van Bogaert Dk, Ogunbanjo GA. Ethics and medicine: Jehovah’s Witnesses and the new blood transfusion rules. S Afr Fam Pract. 2013;55(1):S6-S9.
- West JM. Ethical issues in the care of Jehovah’s Witnesses. Curr Opin Anaesthesiol. 2014;27(2):170-176.
- Beauchamp TL, Childress JF. Principles of Biomedical Ethics. Oxford University Press; 2001.
- Furrow BR, Greaney TL, Johnson SH, et al. Health Law: Cases, Materials and Problems. West; 2013.
- Woolley S. Children of Jehovah’s Witnesses and adolescent Jehovah’s Witnesses: what are their rights? Arch Dis Child. 2005;90(7):715-719.
- Brezina PR, Moskop JC. Urgent medical decision making regarding a Jehovah’s Witness minor: a case report and discussion. N C Med J. 2007;68(5):312-316.
- Simmons FM. The Jehovah’s Witness orthopaedic trauma patient: an ethical challenge. Orthop Nurs. 1999;18(5):28-34.
- Coleman DL, Rosoff PM. The legal authority of mature minors to consent to general medical treatment. Pediatrics. 2013;131(4):786-793.
- The Choice is Not Always Yours: A Minor’s Right to Make Medical Decisions. Campbell Law Observer 2015 [cited 2021 April 9th,]; Available at: http://campbelllawobserver.com/the-choice-is-not-always-yours-a-minors-right-to-make-medical-decisions/.
- Blake V. Minors’ refusal of life-saving therapies. AMA J Ethics. 2012;14(10):792-796.
- Surgeons ACo. Statement on Recommendations for Surgeons Caring for Patients Who Are Jehovah’s Witnesses. Bulletin of the American College of Surgeons 2018 [cited 2021 April 9th]; Available at: https://www.facs.org/about-acs/statements/114-jehovahs.
- Mason CL, Tran CK. Caring for the Jehovah’s witness parturient. Anesth Analg. 2015;121(6):1564-1569.
- Bailey R, Ariga T. The view of Jehovah’s witnesses on blood substitutes. Artif Cells Blood Substit Biotechnol. 1998;26(5-6):571-576.
- Nelson CL, Fontenot HJ. Ten strategies to reduce blood loss in orthopedic surgery. Am J Surg. 1995;170(6):S64-S68.
- Ng T, Marx G, Littlewood T, et al. Recombinant erythropoietin in clinical practice. Postgrad Med J. 2003;79(933):367-376.
- Kuhn V, Diederich L, Keller TCS, et al. Red blood cell function and dysfunction: redox regulation, nitric oxide metabolism, anemia. Antioxid Redox Signal. 2017;26(13):718-742.
- DeLoughery TG. Transfusion replacement strategies in Jehovah’s Witnesses and others who decline blood products. Clin Adv Hematol Oncol. 2020;18(12):826-836.
- Zhao Y, Jiang C, Peng H, et al. The effectiveness and safety of preoperative use of erythropoietin in patients scheduled for total hip or knee arthroplasty: a systematic review and meta-analysis of randomized controlled trials. Medicine (Baltimore). 2016;95(27):e4122.
- Bruce D, Nokes TJC. Prothrombin complex concentrate (Beriplex P/N) in severe bleeding: experience in a large tertiary hospital. Crit Care. 2008;12(4):R105.
- Mauermann WJ, Shilling AM, Zuo Z. A comparison of neuraxial block versus general anesthesia for elective total hip replacement: a meta-analysis. Anesth Analg. 2006;103(4):1018-1025.
- Richman JM, Rowlingson AJ, Maine DN, et al. Does neuraxial anesthesia reduce intraoperative blood loss? A meta-analysis. J Clin Anesth. 2006;18(6):427-435.
- Haughom BD, Schairer WW, Nwachukwu BU, et al. Does neuraxial anesthesia decrease transfusion rates following total hip arthroplasty? J Arthroplasty. 2015;30(Suppl 9):116-120.
- Smith LM, Cozowicz C, Uda Y, et al. Neuraxial and combined neuraxial/general anesthesia compared to general anesthesia for major truncal and lower limb surgery: a systematic review and meta-analysis. Anesth Analg. 2017;125(6):1931-1945.
- Macfarlane AJ, Prasad GA, Chan VWA, et al. Does regional anesthesia improve outcome after total knee arthroplasty? Clin Orthop Relat Res. 2009;467(9):2379-2402.
- Palmer A, Chen A, Matsumoto T, et al. Blood management in total knee arthroplasty: state-of-the-art review. J ISAKOS. 2018;3(6):358-366.
- Poeran J, Rasul R, Suzuki S, et al. Tranexamic acid use and postoperative outcomes in patients undergoing total hip or knee arthroplasty in the United States: retrospective analysis of effectiveness and safety. BMJ. 2014;349:g4829.
- Amer KM, Rehman S, Amer K, et al. Efficacy and safety of tranexamic acid in orthopaedic fracture surgery: a meta-analysis and systematic literature review. J Orthop Trauma. 2017;31(10):520-525.
- Xiao C, Zhang S, Long N, et al. Is intravenous tranexamic acid effective and safe during hip fracture surgery? An updated meta-analysis of randomized controlled trials. Arch Orthop Trauma Surg. 2019;139(7):893-902.
- Zufferey P, Merquiol F, Laporte S, et al. Do antifibrinolytics reduce allogeneic blood transfusion in orthopedic surgery? Anesthesiology. 2006;105(5):1034-1046.
- Pachore JA, Shah VI, Upadhyay S, et al. The use of tranexamic acid to reduce blood loss in uncemented total hip arthroplasty for avascular necrosis of femoral head: a prospective blinded randomized controlled study. Arthroplasty. 2019;1(1):12.
- Manjuladevi M, Upadhyaya KV. Perioperative blood management. Indian J Anaesth. 2014;58(5):573-580.
- Chauncey JM, W.J. Tranexamic Acid. In: StatPearls [Internet]. 2021 [Updated 2021 Mar 2]. [cited 2021 05/01]; Available at: https://www.ncbi.nlm.nih.gov/books/NBK532909/.
- Cheriyan T, Maier SP, Bianco K, et al. Efficacy of tranexamic acid on surgical bleeding in spine surgery: a meta-analysis. Spine J. 2015;15(4):752-761.
- Sethna NF, Zurakowski D, Brustowicz RM, et al. Tranexamic acid reduces intraoperative blood loss in pediatric patients undergoing scoliosis surgery. Anesthesiology. 2005;102(4):727-732.
- Lawson T, Ralph C. Perioperative Jehovah’s Witnesses: a review. Br J Anaesth. 2015;115(5):676-687.
- Bolliger D, Sreeram G, Duncan A, et al. Prophylactic use of factor IX concentrate in a Jehovah’s Witness patient. Ann Thorac Surg. 2009;88(5):1666-1668.
- Aldouri M. The use of recombinant factor VIIa in controlling surgical bleeding in non-haemophiliac patients. Pathophysiol Haemost Thromb. 2002;32(Suppl 1):41-46.
- Shahid A, Khan A. Tranexamic acid in decreasing blood loss during and after caesarean section. J Coll Physicians Surg Pak. 2013;23(7):459-462.
- Sekhavat L, Tabatabaii A, Dalili M, et al. Efficacy of tranexamic acid in reducing blood loss after cesarean section. J Matern Fetal Neonatal Med. 2009;22(1):72-75.
- Muñoz M, García-Erce JA, Villar I, et al. Blood conservation strategies in major orthopaedic surgery: efficacy, safety and European regulations. Vox Sang. 2009;96(1):1-13.
- Kozek-Langenecker SA, Ahmed AB, Afshari A, et al. Management of severe perioperative bleeding: guidelines from the European Society of Anaesthesiology. Eur J Anaesthesiol. 2013;30(6):270-382.
- Fabes J, Brunskill SJ, Curry N, et al. Pro-coagulant haemostatic factors for the prevention and treatment of bleeding in people without haemophilia. Cochrane Database Syst Rev. 2018;12(12):CD010649.
- Franchini M, Lippi G. Fibrinogen replacement therapy: a critical review of the literature. Blood Transfus. 2012;10(1):23-27.
- Mittermayr M, Streif W, Haas T, et al. Hemostatic changes after crystalloid or colloid fluid administration during major orthopedic surgery: the role of fibrinogen administration. Anesth Analg 2007;105(4):905-917, table of contents.
- Fenger-Eriksen C, Jensen TM, Kristensen BS, et al. Fibrinogen substitution improves whole blood clot firmness after dilution with hydroxyethyl starch in bleeding patients undergoing radical cystectomy: a randomized, placebo-controlled clinical trial. J Thromb Haemost. 2009;7(5):795-802.
- Sorensen B, Fries D. Emerging treatment strategies for trauma-induced coagulopathy. Br J Surg. 2012;99(Suppl 1):40-50.
- Carling MS, Zarhoud J, Jeppsson A, et al. Preoperative plasma fibrinogen concentration, factor XIII activity, perioperative bleeding, and transfusions in elective orthopaedic surgery: a prospective observational study. Thromb Res. 2016;139:142-147.
- Beholz S, Liu J, Thoelke R, et al. Use of desmopressin and erythropoietin in an anaemic Jehovah’s Witness patient with severely impaired coagulation capacity undergoing stentless aortic valve replacement. Perfusion. 2001;16(6):485-489.
- Kobrinsky NL, Letts RM, Patel LR, et al. 1-Desamino-8-D-arginine vasopressin (desmopressin) decreases operative blood loss in patients having Harrington rod spinal fusion surgery. A randomized, double-blinded, controlled trial. Ann Intern Med. 1987;107(4):446-450.
- Desborough MJ, Oakland K, Brierley C, et al. Desmopressin use for minimising perioperative blood transfusion. Cochrane Database of Syst Rev. 2017;7(7):CD001884.
- Spahn DR, Bouillon B, Cerny V, et al. The European guideline on management of major bleeding and coagulopathy following trauma: fifth edition. Crit Care. 2019;23(1):98.
- Kwee MM, Ho YH, Rozen WM. The prone position during surgery and its complications: a systematic review and evidence-based guidelines. Int Surg. 2015;100(2):292-303.
- Park CK. The effect of patient positioning on intraabdominal pressure and blood loss in spinal surgery. Anesth Analg. 2000;91(3):552-557.
- Edgcombe H, Carter K, Yarrow S. Anaesthesia in the prone position. Br J Anaesth. 2008;100(2):165-183.
- Kim E, Kim H-C, Lim Y-J, et al. Comparison of intra-abdominal pressure among 3 prone positional apparatuses after changing from the supine to the prone position and applying positive end-expiratory pressure in healthy euvolemic patients: a prospective observational study. J Neurosurg Anesthesiol. 2017;29(1):14-20.
- Lee TC, Yang LC, Chen HJ. Effect of patient position and hypotensive anesthesia on inferior vena caval pressure. Spine (Phila Pa 1976). 1998;23(8):941-947; discussion 947-8.
- Pearce DJ. The role of posture in laminectomy. Proc R Soc Med. 1957;50(2):109-112.
- Akinci IO, Tunali U, Kyzy AA, et al. Effects of prone and jackknife positioning on lumbar disc herniation surgery. J Neurosurg Anesthesiol. 2011;23(4):318-322.
- Shah A, Palmer AJR, Klein AA. Strategies to minimize intraoperative blood loss during major surgery. Br J Surg. 2020;107(2):e26-e38.
- Shander A, Javidroozi M, Perelman S, et al. From bloodless surgery to patient blood management. Mt Sinai J Med. 2012;79(1):56-65.
- Paul JE, Ling E, Lalonde C, et al. Deliberate hypotension in orthopedic surgery reduces blood loss and transfusion requirements: a meta-analysis of randomized controlled trials. Can J Anesth. 2007;54(10):799-810.
- Jiang J, Zhou R, Li B, et al. Is deliberate hypotension a safe technique for orthopedic surgery?: a systematic review and meta-analysis of parallel randomized controlled trials. J Orthop Surg Res. 2019;14(1):409.
- Sum DC, Chung PC, Chen WC. Deliberate hypotensive anesthesia with labetalol in reconstructive surgery for scoliosis. Acta Anaesthesiol Sin. 1996;34(4):203-207.
- Patel NJ, Patel BS, Paskin S, et al. Induced moderate hypotensive anesthesia for spinal fusion and Harrington-rod instrumentation. J Bone Joint Surg Am. 1985;67(9):1384-1387.
- Bansal N, Kaur G, Garg S, et al. Acute normovolemic hemodilution in major orthopedic surgery. J Clin Orthop Trauma. 2020;11(Suppl 5):S844-S848.
- Saricaoglu F, Akinci SB, Celiker V, et al. The effect of acute normovolemic hemodilution and acute hypervolemic hemodilution on coagulation and allogeneic transfusion. Saudi Med J. 2005;26(5):792-798.
- Nishant, Kumari R. Surgical management in treatment of Jehovah’s witness in trauma surgery in Indian subcontinent. J Emerg Trauma Shock. 2014;7(3):215-221.
- Meybohm P, Choorapoikayil S, Wessels A, et al. Washed cell salvage in surgical patients: a review and meta-analysis of prospective randomized trials under PRISMA. Medicine (Baltimore). 2016;95(31):e4490.
- Klein AA, Bailey CR, Charlton AJ, et al. Association of Anaesthetists guidelines: cell salvage for peri-operative blood conservation 2018. Anaesthesia. 2018;73(9):1141-1150.
- Esper SA, Waters JH. Intra-operative cell salvage: a fresh look at the indications and contraindications. Blood Transfus. 2011;9(2):139-147.
- Waters JH, Tuohy MJ, Hobson DF, et al. Bacterial reduction by cell salvage washing and leukocyte depletion filtration. Anesthesiology. 2003;99(3):652-655.
- Kumar N, Zaw AS, Kantharajanna SB, et al. Metastatic efficiency of tumour cells can be impaired by intraoperative cell salvage process: truth or conjecture? Transfus Med. 2017;27(Suppl 5):327-334.
- Cook A, Hanowell LH. Intraoperative autotransfusion for a patient with homozygous sickle cell disease. Anesthesiology. 1990;73(1):177-179.
- Fox JS, Amaranath L, Hoeltge GA, et al. Autologous blood transfusion and intraoperative cell salvage in a patient with homozygous sickle cell disease. Cleve Clin J Med. 1994;61(2):137-140.
- Brajtbord D, Johnson D, Ramsay M, et al. Use of the cell saver in patients with sickle cell trait. Anesthesiology. 1989;70(5):878-878.
- Hulatt LJ, Fisher W. Intra-operative cell salvage and sickle cell carrier status. Anaesthesia. 2010;65(6):649-649.
- Huang L, Liu GL, Kaye AD, et al. Advances in topical hemostatic agent therapies: a comprehensive update. Adv Ther. 2020;37(10):4132-4148.
- Thoms RJ, Marwin SE. The role of fibrin sealants in orthopaedic surgery. J Am Acad Orthop Surg. 2009;17(12):727-736.
- Carvalho MV, Marchi E. Mechanism of action of topical hemostatic and adhesive tissue agents. 2013.
- Brodsky JW, Dickson JH, Erwin WD, et al. Hypotensive anesthesia for scoliosis surgery in Jehovah’s Witnesses. Spine (Phila Pa 1976). 1991;16(3):304-306.
- Ross D, Erkocak O, Rasouli MR, et al. Operative time directly correlates with blood loss and need for blood transfusion in total joint arthroplasty. Arch Bone Jt Surg. 2019;7(3):229-234.
- Bartley CE, Bastrom TP, Newton PO. Blood loss reduction during surgical correction of adolescent idiopathic scoliosis utilizing an ultrasonic bone scalpel. Spine Deform. 2014;2(4):285-290.
- Wahlquist S, Nelson S, Glivar P. Effect of the ultrasonic bone scalpel on blood loss during pediatric spinal deformity correction surgery. Spine Deform. 2019;7(4):582-587.
- Liu H, Liu Z, Zhang Q, et al. Utilization of epinephrine-soaked gauzes to address bleeding from osteotomy sites in non-tourniquet total knee arthroplasty: a retrospective cohort study. BMC Musculoskelet Disord. 2020;21(1):578.
- Zhang Y, Guo W, Tang X, et al. Can aortic balloon occlusion reduce blood loss during resection of sacral tumors that extend into the lower lumber spine? Clin Orthop Relat Res. 2018;476(3):490-498.
- Ullmark G, Hovelius L, Strindberg L, et al. Reduced bleeding through temporary balloon occlusion in hip and knee revision surgery. Acta Orthop Scand. 2000;71(1):51-54.
- Mangar D, Shube S, Omar H, et al. Intravascular balloon to minimize blood loss during total hip replacement in a Jehovah’s Witness. J Clin Anesth. 2011;23(1):71-74.
- DiPasquale T, Greiwe RM, Simmons P, et al. Temporary partial intra-iliac balloon occlusion for the treatment of acetabulum fracture in a Jehovah’s Witness: a case report. J Orthop Trauma. 2005;19(6):415-419.
- Zhang W, Li N, Chen S, et al. The effects of a tourniquet used in total knee arthroplasty: a meta-analysis. J Orthop Surg Res. 2014;9(1):13.
- Smith TO, Hing CB. Is a tourniquet beneficial in total knee replacement surgery? A meta-analysis and systematic review. Knee. 2010;17(2):141-147.
- Huang Z, Xie XW, Li LL, et al. Intravenous and topical tranexamic acid alone are superior to tourniquet use for primary total knee arthroplasty: a prospective, randomized controlled trial. J Bone Joint Surg Am. 2017;99(24):2053-2061.
- Parker MJ, Livingstone V, Clifton R, et al. Closed suction surgical wound drainage after orthopaedic surgery. Cochrane Database Syst Rev. 2007;2007(3):Cd001825.
- Taylor SE, Cross MH. Clinical strategies to avoid blood transfusion. Anaesth Intensive Care Med. 2013;14(2):48-50.
- Ball AM, Winstead PS. Recombinant human erythropoietin therapy in critically Ill Jehovah’s witnesses. Pharmacotherapy. 2008;28(11):1383-1390.
- Schirm S, Scholz M. A biomathematical model of human erythropoiesis and iron metabolism. Sci Rep. 2020;10(1):8602.
- Natanson C, Kern SJ, Lurie P, et al. Cell-free hemoglobin-based blood substitutes and risk of myocardial infarction and death: a meta-analysis. JAMA. 2008;299(19):2304-2312.
- Melmed GM, Hulsey ME, Newhouse M, et al. Clinical strategies for supporting the untransfusable hemorrhaging patient. Bayl Univ Med Cent Proceedings. 2009;22(4):316-320.
- Klein MJ, Carter TI, Smith MC, et al. Prophylactic hypothermia and neuromuscular blockade to limit myocardial oxygen demand in a critically anemic Jehovah’s Witness after emergency surgery. J Surg Case Rep. 2014;2014(12):rju135-rju135.
- Chaney MA, Jellish WS, Leonetti JP. Perioperative management of a Jehovah’s witness presenting for skull base surgery. Skull Base Surg. 1996;6(2):133-136.
- Chand NK, Subramanya HB, Rao GV. Management of patients who refuse blood transfusion. Indian J Anaesth. 2014;58(5):658-664.
- Rajagopalan S, Mascha E, Na J, et al. The effects of mild perioperative hypothermia on blood loss and transfusion requirement. Anesthesiology. 2008;108(1):71-77.
- Fakhry SM, Fata P. How low is too low? Cardiac risks with anemia. Crit Care. 2004;8(Suppl 2):S11.
- Weiskopf RB. Human cardiovascular and metabolic response to acute, severe isovolemic anemia. JAMA. 1998;279(3):217.
- Cunningham AJ. Controlled hypotension to minimize blood loss of anaemic Jehovah’s witness patient undergoing total hip and shoulder replacement. Br J Anaesth. 1982;54(8):895-898.
- Carson J, Noveck H, Berlin JA, et al. Mortality and morbidity in patients with very low postoperative HB levels who decline blood transfusion. Transfusion. 2002;42:812-818.
- Liumbruno G, Bennardello F, Lattanzio A, et al. Recommendations for the transfusion of red blood cells. Blood Transfus. 2009;7(1):49-64.
- Varela JE, Gomez-Marin O, Fleming LE, et al. The risk of death for Jehovah’s Witnesses after major trauma. J Trauma. 2003;54(5):967-972.
- Mihas A, Ramchandran S, Rivera S, et al. Safe and effective performance of pediatric spinal deformity surgery in patients unwilling to accept blood transfusion: a clinical study and review of literature. BMC Musculoskelet Disord. 2021;22(1):204.