
Current Concept Review
Acute Management of Pediatric Knee Dislocations
1Central Texas Pediatric Orthopedics, Dell Medical School, The University of Texas at Austin, Austin, TX; 2Children’s Hospital of the King’s Daughters, Norfolk, VA; 3Monroe Carell Jr. Children’s Hospital at Vanderbilt, Nashville, TN; 4Cincinnati Children’s Hospital, Cincinnati, OH; 5Dell Medical School, The University of Texas at Austin, Austin, TX; 6Children’s Hospital Colorado, Denver, CO; 7Children’s Healthcare of Atlanta, Atlanta, GA
The authors are all members of the Knee Lig RIG in PRISM 
Correspondence: Matthew Ellington, MD, Central Texas Pediatric Orthopedics, 1301 Barbara Jordan Blvd. #300, Austin, TX 78723. E-mail: [email protected]
Received: July 1, 2022; Accepted: July 2, 2022; Published: August 1, 2022
DOI: 10.55275/JPOSNA-2022-0088
Volume 4, Number 3, August 2022
Abstract:
Although pediatric knee dislocations are relatively uncommon, the potential for devastating complications exists. Current treatment has largely been guided by the adult literature as well as small pediatric case series. Early recognition and treatment of vascular injuries is of the utmost importance. Neurological injuries can also lead to devastating long-term complications and therefore prompt recognition is crucial. Ligament reconstruction as opposed to ligament repair has been shown to have improved outcomes in the pediatric population. The subsequent rehabilitation of a child after reconstruction for a knee dislocation also provides a unique challenge. Various sequelae have been described to include neurovascular injuries, residual laxity, and stiffness as well as those unique to pediatric patients such as growth disturbance.
Key Concepts:
- Prompt recognition and reduction of a knee dislocation are imperative.
- Thorough and prompt neurovascular physical examination and consideration of advanced vascular imaging should be performed with any knee dislocation
- After an initial period of immobilization and rehabilitation, stress radiographs play an important role to quantify laxity and guide treatment.
- Ligament reconstruction has been shown to be superior to repair.
Introduction
Knee dislocations are injuries that can be easily missed due to spontaneous reduction of the knee prior to presentation.1,2 They account for only 0.02% of all orthopaedic injuries.1 Currently, most of our knowledge of the management and complications of pediatric knee dislocations comes from small case series and case reports.3–5 While surgical treatment of these injuries can lead to excellent outcomes,6 careful evaluation and management immediately following injury is critical for identifying rare but potentially serious complications, including vascular injury, nerve injury, and compartment syndrome.
Classification
Two main classification systems are used for both adult and pediatric knee dislocations. The first classification system by Kennedy bases the knee dislocation classification off of the position of the tibia relative to the femur (Table 1).7 The second classification system by Schenck, classifies the knee dislocation based on the pattern of injury to the two cruciate ligaments along with the posteromedial and posterolateral corners of the knee (Table 2).8
Table 1. Kennedy Classification of Knee Dislocations7
| Position of the Tibia | Mechanism | Significance |
|---|---|---|
| Anterior | Hyperextension Injury | -Most common -Highest rate of peroneal nerve injury -Arterial injury can occur as an intimal tear due to traction resulting from the hyperextension |
| Posterior | Axial load on a flexed knee, usually a fall or dashboard injury | -2nd Most Common -Highest rate of vascular injury due to complete tear of the popliteal artery |
| Lateral | Varus Force | |
| Medial | Valgus Force | |
| Rotational | Twisting Injury | -May be irreducible if the femoral condyle is button-holed through the capsule -Posterolateral most common direction |
Table 2. Schenck Classification of Knee Dislocations8
| Class | Ligaments Rupture |
|---|---|
| KD I | ACL or PCL with PMC and/or PLC |
| KD II | ACL and PCL only |
| KD IIIM | ACL and PCL with PMC |
| KD IIIL | ACL and PCL with PLC |
| KD IV | ACL, PCL, PMC, and PLC |
| KD V | Multiligamentous Knee Injury with Periarticular Fracture |
| KD = Knee Dislocation ACL = Anterior Cruciate Ligament PCL = Posterior Cruciate Ligament PMC = Posteromedial Corner PLC = Posterolateral Corner |
Acute Presentation and Management
Pediatric knee dislocations can occur during a variety of activities including contact and non-contact sports injuries, trampolines, high-energy trauma such as motor vehicle or ATV accidents, and low-velocity dislocations in morbidly obese patients. Patients may present with an obvious deformity if the knee is still dislocated, but knees that spontaneously reduce or are reduced at the scene of injury may lack an obvious deformity. The pediatric patient with a knee dislocation may present with pain, knee effusion, soft-tissue swelling, ecchymosis, and ligamentous instability. Therefore, any acute knee injury that presents with gross instability and multiple ligaments injured should be worked up in a similar fashion to the dislocated knee.9 Patients presenting from high-energy trauma should also have a thorough trauma evaluation due to the high incidence of head, chest, or abdomen injuries (27%) or other fractures (50–60%).10
After the initial trauma survey and evaluation, a dedicated and focused examination of the entire injured lower extremity should be performed. On first inspection, soft tissue swelling, ecchymosis, joint effusion, and knee joint deformity should be documented. If the knee is still dislocated, the examiner should evaluate for a dimple in the medial or lateral soft tissues which indicates that the femoral condyle may be entrapped in the soft tissues preventing reduction.11
Adequate sedation and traction applied to the dislocated knee are paramount for a successful reduction.1 A thorough sensory and motor exam of the lower extremity is performed before and after the reduction of the dislocated knee. Once reduced, a side-to-side vascular exam should be performed to compare distal extremity palpable pulses and ankle brachial indices (ABIs), with a ratio of 0.9 or greater typically considered to be in the normal range. However, a low threshold should exist to obtain advanced imaging such as a CT angiogram if there is any concern or borderline ABI or altered doppler signals. For those who undergo MRI to assess ligamentous injury, magnetic resonance angiography can also be performed in conjunction with the MRI to evaluate for intimal vascular injuries. In our experience though, CT scan is a quicker evaluation for arterial injury. An examination of the lower extremity compartments should be performed with compartment pressure measurements if there is clinical concern for a compartment syndrome.
If the knee is reduced and there is no concern for vascular injury, a full ligamentous exam should be attempted to evaluate knee stability. Quite often, however, in the acute setting, pain and apprehension limit a full ligamentous exam. The external rotation recurvatum test, whereby the examiner compares the amount of recurvatum between the legs when the great toe is elevated, is one exam that can often be performed in the acute setting with high sensitivity for posterolateral corner injuries (Figure 1).
Figure 1. External rotation recurvatum test is performed to evaluate a patient for posterolateral rotatory instability. One determines if there is an increased knee hyperextension compared to the contralateral side.

A knee spanning external fixator with two half pins in the femur and tibia is reserved for those cases that remain grossly unstable or those that require urgent vascular repair due to an ischemic limb. The rigid fixation allows for protection of the repair and the ability to perform serial neurovascular examinations.1
Imaging
Upon presentation, AP and lateral orthogonal knee x-rays of the affected extremity should be obtained to determine if the knee is reduced. To evaluate for associated fractures, further imaging of the full-length tibia and femur should be obtained once the knee is determined to be reduced. If a reduction is required, post-reduction x-rays should be obtained to confirm reduction before proceeding with advanced imaging (Figure 2A, B). If there is an abnormal palpable or dopplerable pulse or abnormal ankle-brachial index (ABI) following reduction, CT angiography should be obtained to evaluate for vascular injury (Figure 3). CT angiography is the preferred imaging technique due to the ease of obtaining the study and excellent correlation with intraoperative angiography (95%).12
Figure 2. (A) Pre-reduction radiographs of a 13-year-old male with a right knee dislocation. (B) Post-reduction radiographs of a 13-year-old male with a right knee dislocation.
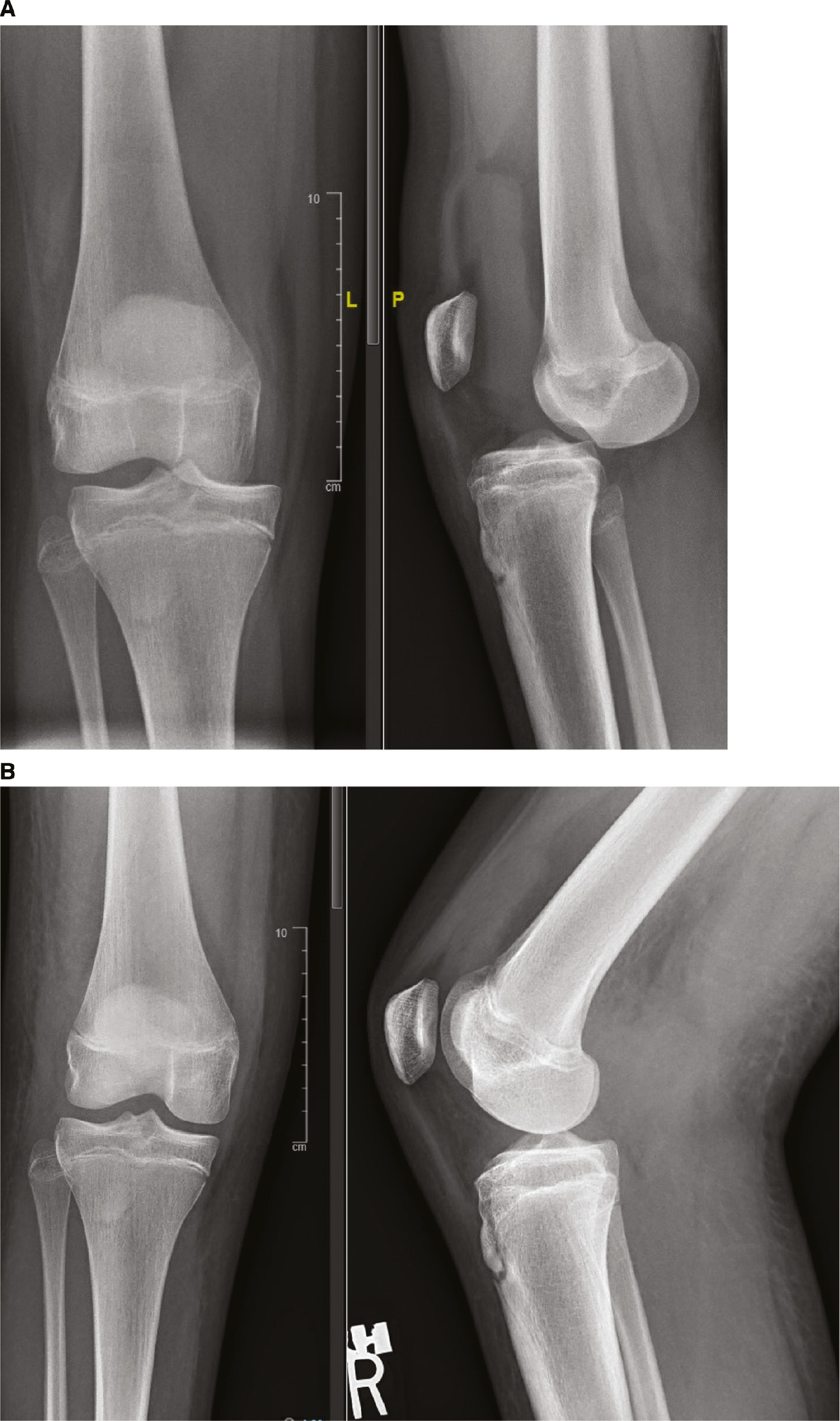
Figure 3. CT angiogram of a patient with a Salter Harris II proximal tibia fracture with an arterial injury.

Magnetic resonance imaging (MRI) should be obtained to confirm ligamentous injury and also to identify associated pathology such as chondral injuries and meniscal tears which have been described to occur in up to 55% of adolescent patients.6 For patients with a normal vascular examination pre- and post-reduction, intimal vascular injuries can still be present, and magnetic resonance angiography can also be performed in conjunction with the MRI. Once knee range of motion is restored and the patient is less guarded, stress radiographs should be obtained to assess laxity of the PCL, medial, and lateral injuries, with the results guiding reconstructive procedures choices.13–15 Relaxation is critical in order to obtain adequate stress radiographs. It may take 2-3 weeks before the patient can relax enough to obtain an adequate stress radiograph.
Vascular Injury
Vascular injuries have been reported to occur in 3.3% to 64% of knee dislocations in the adult literature.16,17 The injury patterns with the highest rates of vascular injuries are KDIII-L knees (32%) and posterior dislocations (25%).18 The risk of vascular injuries in knee dislocations has been reported to be higher in obese patients due to supraphysiologic loads and those with open injuries.19,20 There is a paucity of data in the pediatric population with regards to rates of vascular injuries. A recent study of posterior knee dislocations at pediatric level 1 trauma centers from the American College of Surgeons’ National Trauma Data Set from 2015 to 2016 found vascular injury to occur in 16 (36%) patients with 14 requiring vascular repair. The popliteal artery was injured in two-thirds, with injury to the anterior tibial artery the second most common location for injury.21
The treatment of vascular injuries requires prompt identification. As described in the initial management section, early reduction of the dislocation and notification of the vascular surgery team is of the utmost importance. Pulses should be palpated and an ABI should be obtained to guide treatment. Unrecognized or untreated vascular injuries that result in prolonged limb ischemia can result in amputation.22,23 In contrast to adults, studies suggest that children have fewer associated vascular injuries, but despite this, physicians must be vigilant in assessing for these potentially severe injuries.21 Vascular repair can be challenging in this population, but a recent retrospective review out of a large center found that overall good results can be found in children with vascular trauma treated with revascularization.24
Fasciotomies are rarely necessary following knee dislocations, but in the setting of impending compartment syndrome or following vascular repair with a preceding prolonged ischemia time (greater than 6 hours), may be indicated.
Please see https://bit.ly/3Pv26oy for a more in-depth discussion on the identification and treatment of compartment syndrome for the pediatric patient.25
Nerve Injury
The common peroneal nerve (CPN) is the most commonly injured nerve in the setting of multiligament knee injuries and is especially vulnerable during varus loading to the knee placing the CPN on stretch. Approximately 16-40% of patients with a knee dislocation have a CPN injury.26,27 CPN injury can range from neuropraxia (mild stretching of the nerve with good recovery prognosis), axonotmesis (disruption of axon and myelin with intact perineurium and epineurium), to laceration, nerve rupture, or neurotmesis (complete nerve transection).28 The variety of nerve injuries lead to a variety of treatments and prognoses. It’s important to prescribe an ankle foot orthosis in the instance of a foot drop in order to improve gait and prevent an equinus contracture during treatment and where recovery can be protracted in duration.
Neuropraxia
The initial trauma and forces upon the knee during knee dislocation may stretch the CPN mostly due to its anatomic location being tethered by the proximal fibula. As long as there is no current entrapment or compression of the nerve, nonoperative treatment with watchful waiting and EMG/NCV testing is indicated at 6 weeks, 3 months, and potentially again at 6 months if previous testing is equivacol.26 Spontaneous recovery of CPN injury can occur in 14%-56% of cases,29 with younger patients (<25 years of age) being shown as the only predictor for improved spontaneous recovery.30
Axonotmesis
Axonotmesis is the complete disruption of the nerve axon and surrounding myelin, but the perineurium and epineurium are left intact.31 This can occur with nerve incarceration in a fracture, with hematoma compression, or when the nerve is entrapped in scar tissue and undergoes a stretch mechanism. Any time the cause of nerve injury is identified to be irreversible, treatment may be indicated with nerve exploration and neurolysis. Preoperative work-up with magnetic resonance imaging (MRI) and or ultrasonography aids in surgical planning identifying the location of nerve injury as well as compression site and/or cause. While neurolysis at the time of acute ligamentous reconstruction may have improved functional outcomes, several studies have shown an improvement in Medical Research Council (MRC) grades from 0 to at least a 4 (Table 3) even with neurolysis after 3 months and in some cases after 7 months32,33
Table 3. Medical Research Council (MRC) Grading System
| Medical Research Council Grading System | |
|---|---|
| Grade | Description |
| 0 | No contraction |
| 1 | Flicker or trace of contraction |
| 2 | Active movie with gravity eliminated |
| 3 | Active movement against gravity |
Length of nerve injury also plays a role in treatment indications and prognosis with longer areas of injury potentially requiring excision and grafting or nerve transfer.26 Larger gaps to span (> 6cm) have also been seen to have declining functional outcomes and poorer prognosis.33–35
Neurotmesis
A complete disconnection or disruption of the nerve occurs in neurotmesis and treatment choice is dictated by the length of disruption.31 Direct end-to-end tensionless repair is the preferred method of treatment for complete disruption; however, direct repair is not always possible in the setting of knee dislocations due to the high likelihood of associated stretch injury.26 Additionally, outcomes of direct repair of the nerve are supported by many authors to have the best outcomes when performed within the 3 to 6-month time frame.26,35 Nerve conduit, or semi-rigid cylindrical tubes usually made of synthetic polyester-based sources, have shown comparable outcomes to direct repair in discontinuity of gaps that are 3-4 cm long.31
A nerve graft is recommended when a gap in the nerve is greater than 2 cm, the direct repair proves to be under tension, or the treatment time frame has been delayed > 6 months. Grafting can be performed with either a cable graft, trunk graft, or when the distance to span is greater than 6 cm, a vascularized nerve graft may be performed.31
Postoperatively, a Tinel’s over the peroneal nerve can be tracked distally and recorded as a distance from the fibular head as a sign of progressive nerve recovery. Finally, tendon transfer or ankle-foot orthoses tend to be reserved for irreparable injuries as well as nerve injuries that have failed other attempts at repair and/or once time-dependent myoneural degeneration has occurred. For the CPN, equinovarus deformity tends to be the resulting foot position and posterior tibial tendon transfer (PTTT) is the recommended treatment. It has been shown that patients who undergo PTTT are able to return to ambulation without an ankle foot orthosis, regardless of the timing of treatment, but more needs to be learned about the ability of these patients to return to athletic activity.26,28
Surgical Reconstruction
Multiligament knee injuries secondary to traumatic knee dislocations result in a variety of injury patterns. Ligament reconstruction is guided by preoperative assessment of laxity and imaging.
Some posterior cruciate ligament (PCL) and medial knee injuries are amenable to nonoperative treatment following an initial 6 weeks of brace immobilization. For this reason, preoperative stress radiographs (varus, valgus, and/or posterior drawer based on injury pattern) should be performed to quantify laxity and guide treatment of collateral and PCL injuries. Stress radiographs have been validated and described in detail by LaPrade et al.14,15 and Jackman et al.26
There are several key principles to multiligament knee reconstruction.
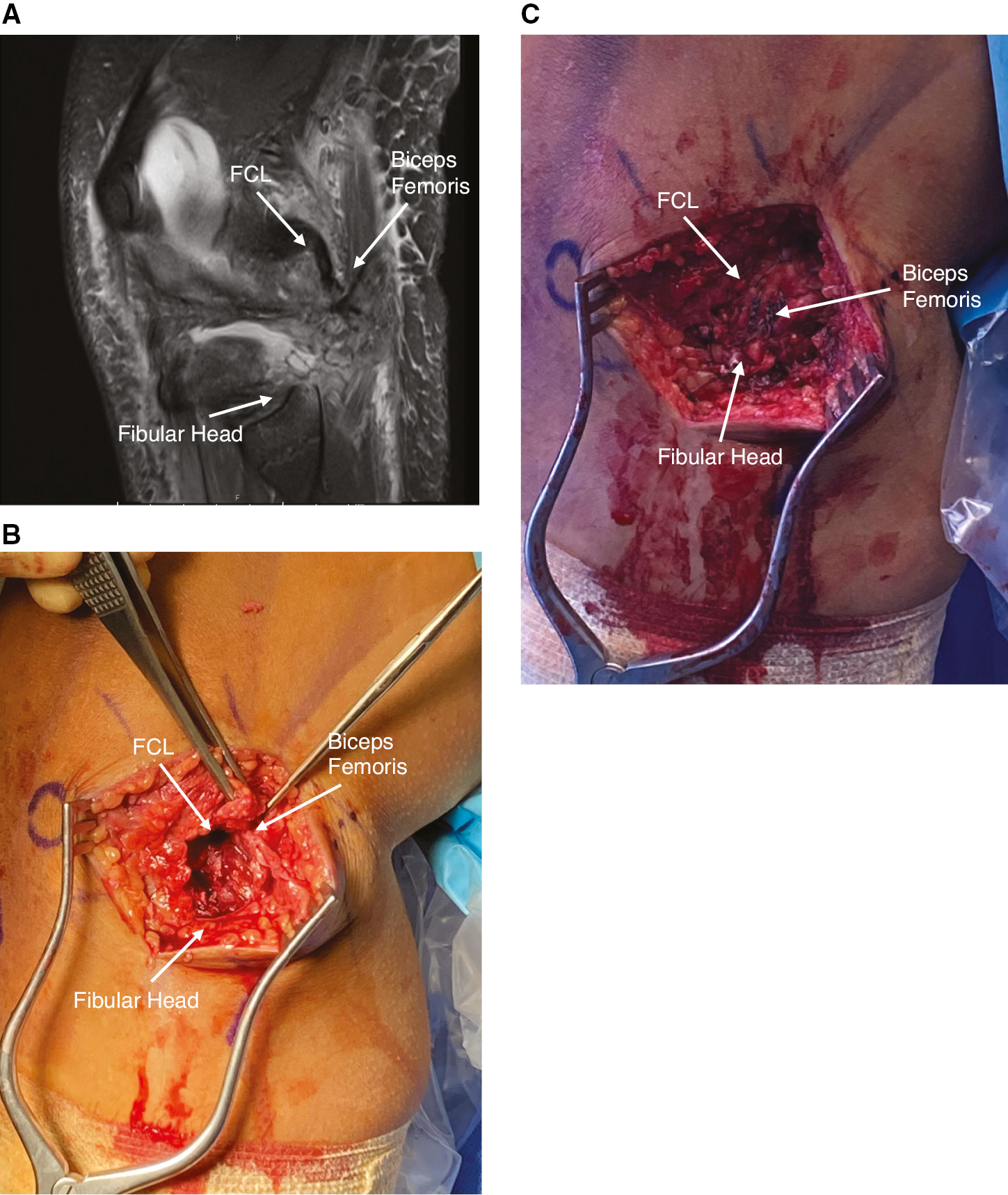
- Ligament reconstruction restores native knee stability with lower rates of failure as compared to repair.36–40 Primary repair within 3 weeks of injury should be reserved for a small subset of avulsion injuries, most notably bony avulsions without mid-substance ligament tearing or attenuation (Figures 4 and 5A, B, C).
- Anatomic reconstruction techniques restore biomechanics and allow early postoperative knee range of motion with improved outcomes and stability and lower rates of arthrofibrosis as compared to non-anatomic reconstruction techniques.36,41,42,43
- Single-stage reconstructions are favored to allow early knee range of motion and to avoid non-physiologic loading of reconstructed grafts in the setting of other non-reconstructed ligaments.44–46
- Autograft ACL reconstruction has significantly lower rates of graft failure as compared to allograft.47–49 Double-bundle or single-bundle PCL reconstruction, posterolateral corner, and posteromedial corner reconstructions can be performed with allograft in the adolescent patient population with acceptable outcomes.6,50
Figure 4. Bony avulsion of fibular collateral ligament (FCL) and popliteus from lateral femoral condyle in a 13-year-old male.

Figure 5 A, B, C. Bony avulsion of the biceps femoris and FCL from the proximal fibula and associated open repair with suture anchors in a 14-year-old male after a football injury.
PCL reconstruction is performed for those injuries with significant instability despite initial conservative management. Reconstruction of both the anterolateral and posteromedial bundles via a double-bundle ACL reconstruction has been demonstrated to improve knee kinematics and patient outcomes as compared to prior single-bundle reconstruction techniques.51 This is performed utilizing a single-transtibial tunnel and two femoral sockets in the center of the bundle footprints.52
Anatomic posterolateral corner reconstruction has been described in detail and validated by Robert LaPrade.53 Peroneal nerve neurolysis is a critical component of the procedure and necessary for the safe drilling of an anatomic FCL tunnel in the fibula as well as to minimize the risk of peroneal nerve neuropraxia postoperatively. Tunnel convergence between the FCL and ACL femoral tunnels can be avoided by aiming the FCL femoral tunnel approximately 35 degrees anteriorly.54
In patients with a peroneal nerve palsy resulting from their initial injury, the peroneal nerve is typically in continuity but can be significantly enlarged and encased in adhesions. Meticulous peroneal nerve neurolysis and decompression can be followed by the use of a nerve wrap to prevent further adhesions. Alternatively, if complete disruption is anticipated, operative treatment should be done in conjunction with a microvascular surgeon.
Medial knee injuries, which fail to improve with bracing and have valgus instability in both flexion and extension, are treated with anatomic MCL and posterior oblique ligament (POL) reconstructions.55 To avoid convergence between the superficial MCL, POL, and PCL tunnels, the superficial MCL femoral tunnel is aimed 40 degrees proximally and anteriorly and the POL tunnel 20 degrees proximally and anteriorly.
Rehabilitation Considerations after Pediatric Knee Dislocation
Multiple factors are considered when deciding on the surgical approach to acute knee dislocations in the pediatric population. Likewise, the rehabilitation of a young patient after surgical repair or reconstruction of a knee dislocation is highly variable. Early stages of rehabilitation depend on the following factors: structures injured, structures reconstructed and/or repaired, and overall knee stability. The rehabilitation process should include pre-surgery rehabilitation, when possible, to gain maximum ROM and quad function and establish postoperative expectations. The aims of postoperative rehabilitation are to minimize complications such as failure of repaired and reconstructed structures, arthrofibrosis, prolonged weakness, knee instability, or failure to return to activities.
Repair Specific Considerations
In the early stages of rehabilitation, weight-bearing status and ROM restrictions are guided by the surgical procedure performed, making postoperative communication between the surgeon and physical therapist of utmost importance. For anatomic posterior cruciate ligament (PCL), posterolateral corner, and medial-sided reconstructions, early initiation of physical therapy for range of motion and quadriceps control is important. In 2008, a systematic review found that early rehabilitation (starting prior to 3 weeks) led to better results in regard to ROM, knee stability, and outcome scores than delaying rehab until after 3 weeks.56 In 2017, Lynch et al. developed a criterion-based progression for multiligament rehabilitation based on (1) tissue protection, (2) restoration of motor control, and (3) optimization of function as well as modifications based on individual surgical procedures.46 The tissue repair with the greatest chance of failure or complication is often the rate-limiting factor in postoperative rehabilitation.57
Range of Motion Restrictions
In a patient with PCL or PLC reconstruction, ROM is typically limited to 0-90 degrees for the first 2 to 4 weeks to protect grafts, and range of motion is typically done passively.58 Care must also be taken to avoid posterior glide of the tibia with knee extension as this can stress the PCL, FCL, and posterolateral corner grafts in the early stages. The physical therapist may need to provide an anterior glide to the tibia or perform ROM in prone position to avoid posterior tibial translation associated with supine ROM.57 Patients with biceps femoris repairs should avoid active contractions of the hamstrings in the first 6 weeks again requiring knee flexion to be done passively. Towel-assisted heel slides, wall slides, or other techniques can be used to avoid recruiting the hamstrings. In patients with PCL and posterolateral corner repairs, care should also be taken to avoid hyperextension of the knee for the first few weeks as well to reduce tension repaired structures that naturally resist knee hyperextension.58 Full knee extension remains critical and can be obtained early with patellofemoral mobilizations and active quad sets.
For patients who have undergone meniscus repairs, there is limited evidence to support postoperative recommendations. Consideration should be taken to avoid knee flexion past 90 degrees in the initial postoperative period depending on the type of meniscus repair.57
Weight-Bearing Restrictions
Weight-bearing restrictions vary considerably between type of repair or reconstruction and surgeon preference. Lynch et al. found the literature to be inconsistent for postoperative weight-bearing restrictions after meniscus repair.57 Typically, reconstructions including the PCL and collateral ligaments are recommended to be toe-touch weight or heel touch bearing for 6 weeks with a brace locked in extension, with progressive weight-bearing beginning in weeks 6 and 7. This approach allows for the benefits of partial weight-bearing, such as chondral and meniscal nutrition and quadriceps function, while limiting stress on the graft reconstructions. At 6 weeks, postop the brace can be unlocked for ambulation if range of motion, motor control, and strength are sufficient. The author’s preference is for patients to be able to perform a minimum of 10 repetitions of straight leg raise without any extension lag prior to increasing available flexion ROM of the postop brace to avoid walking with a flexed knee gait.
Strengthening Progression
The goals of strengthening in the multiligament postoperative patient are to improve neuromuscular control progressively while respecting healing tissues. The progression for knee neuromuscular rehabilitation is isometric exercises (quad sets, multi-angle isometrics, etc.), open chain strengthening (straight leg raise in different planes, resisted knee extension in limited motion, etc.), bilateral and unilateral WB exercises (wall squats, chair squats, step-ups, etc.), and finally, more traditional strength training and plyometrics closer to return to activities (squats, deadlifts, squat jumps, etc.). The early stages of this progression will focus on endurance with higher repetitions of exercises then progressing to strength and power development later in rehab. Attention to proper form will help the patient avoid compensatory movements while strengthening.
Authors Preferred Guidelines Post Multiligament Reconstruction
| Time Frame | Special Precautions | ROM Goals | Exercise Progression |
|---|---|---|---|
| 0-6 weeks | -flexion 0-90 for the first 2-4 weeks -no passive hyperextension for 4-6 weeks -avoid posterior tibial translation 6 weeks -no isolated hamstring work in biceps femoris repair for 8 weeks |
-flexion 0-90 by 4 weeks and 115 by 6 weeks -full extension by 6 weeks |
-isometric exercises progressing to limited ROM open chain strengthening focusing on quad recovery and lateral hip strength where allowed |
| 6-16 weeks | -limit FWB strengthening to 0-70 degrees flexion early in this phase -no open chain isolated hamstring work in PCL or posterolateral corner reconstructions |
-flexion and extension equal to contralateral knee | -bilateral then progress to unilateral FWB strengthening exercises within restrictions |
| 4-6 months | -slow progression from jogging to straight line running to sprinting with attention to swelling or pain | -full ROM during functional tasks and strengthening | -focus on building strength, power, and mass with varying rep and set ranges as well as higher loads -make use of isometric, concentric, and eccentric exercises |
| 6-9 months | -initiate cutting, pivoting, and sports-specific activities with attention to proper form and control and reducing compensatory movement patterns |
Return to Sport
Return to sport timelines after knee dislocation and multiligament knee reconstruction is typically no sooner than 9-12 months. Return to play considerations should include not only chronological time, but also depends on a comprehensive evaluation to look for limb symmetry, strength, and dynamic control during high-level tasks. The authors find the following tests helpful in determining return to sport readiness: isokinetic or hand-held dynamometer testing for strength and limb symmetry, Y-balance test, single-leg hop test, triple hop test, crossover hop test, and 6-meter hop. All of these should be achieved at a level of 90% or better and have good form and control to be considered passing. It is also suggested that psychological readiness is considered with the use of a validated form such as the ACL-Return to Sport after Injury (ACL-RSI).59
Sequelae and Its Management
Functional Outcomes
Concomitant neurovascular injuries, including popliteal artery injuries requiring repair and complete peroneal nerve palsies, have the potential to dramatically impact both short- and long-term outcomes. Several studies have reported satisfactory subjective and objective outcomes after dislocation at short-, mid-, and long-term follow-up, using various patient-reported outcome measures.6,60–63 Such studies are often in adult populations and limited by the heterogeneity of pathology that occurs concomitant to knee dislocations. Surgical technique, involved ligamentous injuries, and rehabilitation protocols often vary widely in these outcome studies. Literature in the adult population suggests that acute ligamentous reconstruction after knee dislocation yields favorable results in terms of basic knee function and activities of daily living. Return to previous level of athletic activity can be less predictable with high rates of osteoarthritis reported at long-term follow-up.1,63
LaPrade et al. conducted a retrospective review of 20 adolescent patients who underwent multiligament knee reconstruction with a minimum 2-year follow-up. Patients’ WOMAC, Lysholm, and SF-12 scores improved significantly postoperatively. There was no difference in patient-reported outcomes between acute ligamentous reconstruction (< 6 weeks) and chronic reconstruction (> 6 weeks).6 95% of patients returned to the same level of sport. None of the patients had arthrofibrosis, infection, or deep vein thrombosis. These results mirror those in the adult literature and are supported by similar series in pediatric patients.50
Growth Disturbance
Pediatric patients who sustain knee dislocations are at risk for physeal disturbance and growth arrest. Knee dislocations in this population are commonly high-energy injuries and, thus, confer risk to the surrounding physes if they have associated physeal fractures. This can include limb length discrepancy due to physeal arrest or angular deformity as a result of physeal disturbance. Genu recurvatum secondary to tibial tubercle apophyseal arrest can also occur.6 Data on the incidence and severity of growth disturbance after knee dislocation in children are lacking. In pure dislocations, reconstructive efforts must take into consideration physeal sparing techniques to decrease the potential for iatrogenic injury.
Ligamentous reconstruction after pediatric knee dislocation must also account for and protect the physes about the knee.3 For skeletally immature patients with significant growth remaining, physeal sparing, partial transphyseal, and transphyseal reconstruction techniques have been described. In a review of ligament reconstruction after multiligamentous, PCL-based injuries in adolescents; Fanelli et al. found no postoperative growth arrest or angular deformity in long-term follow-up.50,63
Loss of Motion
Arthrofibrosis after knee dislocation, particularly after multiligament reconstruction, is a common problem. The diffuse nature of the soft tissue injury in knee dislocations predisposes to fibrosis and scar formation.64 Rehabilitation protocols should prioritize optimization of preoperative range of motion in order to maximize functional outcomes after surgery. Postoperative stiffness can be due to a variety of factors, including intraarticular adhesions formation, graft placement and tensioning issues, and timing of surgery.64 The rate of arthrofibrosis has not been documented in the literature, but studies have shown the most significant risk factors for stiffness to be multiligamentous knee injury, knee dislocation, and the use of an external fixator.65 Persistent fibrosis may require manipulation under anesthesia or repeat arthroscopy for lysis of adhesions with success rates up to 90%.66
Residual Laxity
Residual ligamentous laxity following anatomic reconstruction and appropriate physical therapy is unusual. However, recurrent instability can occur and is most often due to technical errors in graft placement or noncompliance with postoperative restrictions.64 As in single-ligament reconstructions, anatomic and isometric restoration of each ligament disrupted after knee dislocation is key to restoring proper biomechanics. Posterior laxity has been reported most commonly in the literature.62,67 This is thought to be multifactorial, possibly due to the difficulty inherent in reconstructing the unique anatomy of the PCL. Proper identification and treatment of all ligamentous pathology resultant from a knee dislocation are necessary in order to ensure postoperative stability. Missed medial collateral ligament injuries or posterolateral corner injuries can increase forces on other reconstructed grafts and lead to postoperative instability and subsequent graft failure unless properly identified and addressed at the index procedure.68
Summary
The prompt recognition and treatment of pediatric knee dislocations are paramount to preventing potentially devastating complications. Initial assessment of the neurovascular status of the limb followed by appropriate reconstruction versus repair guide our treatment of this rare condition. The rehabilitation of these injuries provides another unique challenge as well. Currently, most of the literature to guide treatment comes from adult literature. More pediatric-specific studies are needed to help in guiding treatment as well as better describing the natural history of the condition.
References
- Rihn JA, Groff YJ, Harner CD, et al. The acutely dislocated knee: evaluation and management. J Am Acad Orthop Surg. 2004;12(5):334–346.
- Sillanpää PJ, Kannus P, Niemi ST, et al. Incidence of knee dislocation and concomitant vascular injury requiring surgery: a nationwide study. J Trauma Acute Care Surg. 2014;76(3):715-719.
- Flowers A, Copley LAB. High-energy knee dislocation without anterior cruciate ligament disruption in a skeletally immature adolescent. Arthroscopy. 2003;19(7):782-786.
- Kwolek CJ, Sundaram S, Schwarcz TH, et al. Popliteal artery thrombosis associated with trampoline injuries and anterior knee dislocations in children. Am Surg. 1998;64(12):1183-1187.
- Witz M, Witz S, Tobi E, et al. Isolated complete popliteal artery rupture associated with knee dislocation. Case reports. Knee Surg Sports Traumatol Arthrosc. 2004;12(1):3-6.
- Godin JA, Cinque ME, Pogorzelski J, et al. Multiligament knee injuries in older adolescents: a 2-year minimum follow-up study. Orthop J Sports Med. 2017;5(9).
- Kennedy JC. Complete dislocation of the knee joint. J Bone Joint Surg Am. 1963;45:889-904.
- Schenck RC Jr, Hunter RE, Ostrum RF, et al. Knee dislocations. Instr Course Lect. 1999;48:515-522.
- McDonough EB Jr, Wojtys EM. Multiligamentous injuries of the knee and associated vascular injuries. Am J Sports Med. 2009;37(1):156-159.
- Wascher DC. High-velocity knee dislocation with vascular injury. Treatment principles. Clin Sports Med. 2000;19(3):457-477.
- Mayer S, Albright JC, Stoneback JW. Pediatric knee dislocations and physeal fractures about the knee. J Am Acad Orthop Surg. 2015;23(9):571-580.
- Seamon MJ, Smoger D, Torres DM, et al. A prospective validation of a current practice: the detection of extremity vascular injury with CT angiography. J Trauma. 2009;67(2):238-243; discussion 243-244.
- Hewett TE, Noyes FR, Lee MD. Diagnosis of complete and partial posterior cruciate ligament ruptures. Stress radiography compared with KT-1000 arthrometer and posterior drawer testing. Am J Sports Med. 1997;25(5):648-655.
- Laprade RF, Bernhardson AS, Griffith CJ, et al. Correlation of valgus stress radiographs with medial knee ligament injuries: an in vitro biomechanical study. Am J Sports Med. 2010;38(2):330-338.
- LaPrade RF, Heikes C, Bakker AJ, et al. The reproducibility and repeatability of varus stress radiographs in the assessment of isolated fibular collateral ligament and grade-III posterolateral knee injuries. An in vitro biomechanical study. J Bone Joint Surg Am. 2008;90(10):2069-2076.
- Chowdhry M, Burchette D, Whelan D, et al. Knee dislocation and associated injuries: an analysis of the American College of Surgeons National Trauma Data Bank. Knee Surg Sports Traumatol Arthrosc. 2020;28(2):568-575.
- Natsuhara KM, Yeranosian MG, Cohen JR, et al. What is the frequency of vascular injury after knee dislocation? Clin Orthop Relat Res. 2014;472(9):2615-2620.
- Medina O, Arom GA, Yeranosian MG, et al. Vascular and nerve injury after knee dislocation: a systematic review. Clin Orthop. 2014;472(9):2621-2629.
- Weinberg DS, Scarcella NR, Napora JK, et al. Can vascular injury be appropriately assessed with physical examination after knee dislocation? Clin Orthop Relat Res. 2016;474(6):1453-1458.
- Henrichs A. A review of knee dislocations. J Athl Train. 2004;39(4):365-369.
- Parrado RH, Notricia DM. Vascular and neurological injury in children with posterior traumatic knee dislocation. Am Surg. 2021;0(0):1-3.
- Parker S, Handa A, Deakin M, et al. Knee dislocation and vascular injury: 4 year experience at a UK Major Trauma Centre and vascular hub. Injury. 2016;47(3): 752-756.
- Downs AR, MacDonald P. Popliteal artery injuries: civilian experience with sixty-three patients during a twenty-four year period (1960 through 1984). J Vasc Surg. 1986;4(1):55-62.
- Kirkilas M, Notrica DM, Langlais CS, et al. Outcomes of arterial vascular extremity trauma in pediatric patients. J Pediatr Surg. 2016;51(11):1885-1890.
- Souder C, Yang S, Greenhill D, et al. Pediatric acute compartment syndrome. JPOSNA®. 2021;3(2).
- Mook WR, Ligh CA, Moorman CT 3rd, et al. Nerve injury complicating multiligament knee injury: current concepts and treatment algorithm. J Am Acad Orthop Surg. 2013;21(6):343-354.
- LaPrade RF. Complications associated with posterolateral knee injuries. In: Posterolateral Knee Injuries: Anatomy, Evaluation and Treatment. New York, NY: Thieme; 2006:214-226.
- Johnson ME, Foster L, DeLee JC. Neurologic and vascular injuries associated with knee ligament injuries. Am J Sports Med. 2008;36(12):2448-2462.
- Plancher KD, Siliski J. Long-term functional results and complications in patients with knee dislocations. J Knee Surg. 2008;21(4):261-268.
- Peskun CJ, Chahal J, Steinfeld ZY, et al. Risk factors for peroneal nerve injury and recovery in knee dislocation. Clin Orthop Relat Res. 2012;470(3):774-778.
- Bhandari PS. Management of peripheral nerve injury. J Clin Orthop Trauma. 2019;10(5):862-866.
- Thoma A, Fawcett S, Ginty M, et al. Decompression of the common peroneal nerve: experience with 20 consecutive cases. Plast Reconstr Surg. 2001;107(5): 1183-1189.
- Seidel JA, Koenig R, Antoniadis G, et al. Surgical treatment of traumatic peroneal nerve lesions. Neurosurgery. 2008;62(3):664-673.
- Kim DH, Murovic JA, Tiel RL, et al. Management and outcomes in 318 operative common peroneal nerve lesions at the Louisiana State University Health Sciences Center. Neurosurgery. 2004;54(6):1421-1428, discussion 1428-1429.
- Giuseffi SA, Bishop AT, Shin AY, et al. Surgical treatment of peroneal nerve palsy after knee dislocation. Knee Surg Sports Traumatol Arthrosc. 2010;18(11):1583-1586.
- Geeslin AG, LaPrade RF. Outcomes of treatment of acute grade-III isolated and combined posterolateral knee injuries: a prospective case series and surgical technique. J Bone Joint Surg Am. 2011;93:1672-1683.
- Levy BA, Dajani KA, Morgan JA, et al. Repair versus reconstruction of the fibular collateral ligament and posterolateral corner in the multiligament-injured knee. Am J Sports Med. 2010;38:804-809.
- LaPrade RF, Johansen S, Agel J, et al. Outcomes of an anatomic posterolateral knee reconstruction. J Bone Joint Surg Am. 2010;92:16-22.
- Wijdicks CA, Michalski MP, Rasmussen MT, et al. Superficial medial collateral ligament anatomic augmented repair versus anatomic reconstruction: an in vitro biomechanical analysis. Am J Sports Med. 2013;41:2858-2866.
- Black BS, Stannard JP. Repair versus reconstruction in acute posterolateral instability of the knee. Sports Med Arthrosc Rev. 2015;23:22-26.
- Jackman T, LaPrade RF, Pontinen T, et al. Intraobserver and interobserver reliability of the kneeling technique of stress radiography for the evaluation of posterior knee laxity. Am J Sports Med. 2008;36:1571-1576.
- Laprade RF, Wijdicks CA. Surgical technique: development of an anatomic medial knee reconstruction. Clin Orthop Relat Res. 2012;470:806-814.
- LaPrade RF, Spiridonov SI, Coobs BR, et al. Fibular collateral ligament anatomical reconstructions: a prospective outcomes study. Am J Sports Med. 2010;38:2005-2011.
- LaPrade RF, Muench C, Wentorf F, et al. The effect of injury to the posterolateral structures of the knee on force in a posterior cruciate ligament graft: a biomechanical study. Am J Sports Med. 2002;30:233-238.
- LaPrade RF, Resig S, Wentorf F, et al. The effects of grade III posterolateral knee complex injuries on anterior cruciate ligament graft force. A biomechanical analysis. Am J Sports Med. 1999;27:469-475.
- Levy BA, Dajani KA, Whelan DB, et al. Decision making in the multiligament-injured knee: an evidence-based systematic review. Arthroscopy. 2009;25:430-438.
- DeFrancesco CJ, Striano BM, Bram JT, et al. An in-depth analysis of graft rupture and contralateral anterior cruciate ligament rupture rates after pediatric anterior cruciate ligament reconstruction. Am J Sports Med. 2020;48:2395-2400.
- Engelman GH, Carry PM, Hitt KG, et al. Comparison of allograft versus autograft anterior cruciate ligament reconstruction graft survival in an active adolescent cohort. Am J Sports Med. 2014;42:2311-2318.
- Kaeding CC, Aros B, Pedroza A, et al. Allograft versus autograft anterior cruciate ligament reconstruction: predictors of failure from a MOON prospective longitudinal cohort. Sports Health. 2011;3:73-81.
- Fanelli GC, Fanelli DG. Knee dislocations and PCL-based multiligament knee injuries in patients aged 18 years and younger: surgical technique and outcomes. J Knee Surg. 2016;29(4):269-277.
- Chahla J, Moatshe G, Cinque ME, et al. Single-bundle and double-bundle posterior cruciate ligament reconstructions: a systematic review and meta-analysis of 441 patients at a minimum 2 years’ follow-up. Arthroscopy. 2017;33:2066-2080.
- Chahla J, Nitri M, Civitarese D, et al. Anatomic double-bundle posterior cruciate ligament reconstruction. Arthrosc Tech. 2016;5:e149-e156.
- Serra Cruz R, Mitchell JJ, Dean CS, et al. Anatomic posterolateral corner reconstruction. Arthrosc Tech. 2016;5:e563-e572.
- Moatshe G, Brady AW, Slette EL, et al. Multiple ligament reconstruction femoral tunnels: intertunnel relationships and guidelines to avoid convergence. Am J Sports Med. 2017;45:563-569.
- Coobs BR, Wijdicks CA, Armitage BM, et al. An in vitro analysis of an anatomical medial knee reconstruction. Am J Sports Med 2010;38:339-347.
- Mook WR, Miller MD, Diduch DR, et al. Multiple-ligament knee injuries: a systematic review of the timing of operative intervention and postoperative rehabilitation. J Bone Joint Surg Am. 2009;91(12):2946-2957.
- Lynch AD, Chmielewski T, Bailey L, et al. STaR Trial Investigators. Current concepts and controversies in rehabilitation after surgery for multiple ligament knee injury. Curr Rev Musculoskelet Med. 2017;10(3):328-345.
- Monson J, Schoenecker J, Schwery N, et al. Postoperative rehabilitation and return to sport following multiligament knee reconstruction. Arthrosc Sports Med Rehabil. 2022;4(1):e29-e40.
- Brinlee AW, Dickenson SB, Hunter-Giordano A, et al. ACL reconstruction rehabilitation: clinical data, biologic healing, and criterion-based milestones to inform a return-to-sport guideline. Sports Health. 2021:19417381211056873.
- Harner CD, Waltrip RL, Bennett CH, et al. Surgical management of knee dislocations. J Bone Joint Surg Am. 2004;86(2):262-273.
- Noyes FR, Barber-Westin SD. Reconstruction of the anterior and posterior cruciate ligaments after knee dislocation. Use of early protected postoperative motion to decrease arthrofibrosis. Am J Sports Med. 1997;25(6):769-778.
- Shapiro MS, Freedman EL. Allograft reconstruction of the anterior and posterior cruciate ligaments after traumatic knee dislocation. Am J Sports Med. 1995;23(5):580-587.
- Fanelli GC, Sousa PL, Edson CJ. Long-term followup of surgically treated knee dislocations: stability restored, but arthritis is common. Clin Orthop Relat Res. 2014;472(9):2712-2717. doi:10.1007/s11999-014-3707-6.
- Hegyes MS, Richardson MW, Miller MD. Knee dislocation. Complications of nonoperative and operative management. Clin Sports Med. 2000;19(3):519-543.
- Bodendorfer BM, Keeling LE, Michaelson EM, et al. Predictors of knee arthrofibrosis and outcomes after arthroscopic lysis of adhesions following ligamentous reconstruction: a retrospective case-control study with over two years’ average follow-up. J Knee Surg. 2019;32(6):536-543.
- Fabricant PD, Tepolt FA, Kocher MS. Range of motion Improvement following surgical management of knee arthrofibrosis in children and adolescents. J Pediatr Orthop. 2018;38(9):e495-e500.
- Thomsen PB, Rud B, Jensen UH. Stability and motion after traumatic dislocation of the knee. Acta Orthop Scand. 1984;55(3):278-283.
- Harner CD, Irrgang JJ, Paul J, et al. Loss of motion after anterior cruciate ligament reconstruction. Am J Sports Med. 1992;20(5):499-506.