
Current Concept Review
A Practical Guide for Improving Orthopaedic Care in Children with Autism Spectrum Disorder
1Department of Orthopaedics & Rehabilitation, Yale School of Medicine, New Haven, CT; 2Child Study Center, Yale School of Medicine, New Haven, CT; 3Department of Pediatrics, Yale School of Medicine, New Haven, CT
Correspondence: David B. Frumberg, MD, P.O. Box 208071, New Haven, CT 06520-8071. E-mail: [email protected]
Received: December 20, 2022; Accepted: December 30, 2022; Published: February 1, 2023
Volume 5, Number 1, February 2023
Abstract
Given the increasing prevalence of autism spectrum disorder (ASD), medical professionals’ understanding of the presentation of ASD is essential to ensuring patients with ASD receive high-quality healthcare. Previous studies have found that individuals with ASD have a lower average bone density and higher fracture risk than those without ASD, increasing the likelihood that these patients will seek orthopaedic care. Early coordination with the patient’s family, identification of stressors and coping strategies, and flexibility during the visit are key to promoting a positive medical encounter. Based on a review of the literature, we present a practical guide for orthopaedic providers to better care for pediatric patients with ASD and their families.
Key Concepts
- Children with ASD have more successful interfaces with pediatric orthopedists when the visits are tailored to meet their unique needs.
- A multidisciplinary team, especially with ASD resources, can improve the experience of surgical admissions.
- A phone call by a team member prior to an outpatient visit is an efficient way to ensure all of a child’s needs will be met.
- Children may have nonverbal communication strategies, including challenges in externalizing pain.
Introduction
Autism spectrum disorder (ASD) is a neurodevelopmental disorder with variable clinical presentations, generally characterized by difficulties with social interaction and communication, as well as restricted or repetitive patterns of thoughts and behaviors.1 Within the past 2 decades, the prevalence of ASD in the pediatric population in the United States has risen from 1 in 150 children in 2000 to 1 in 40 children in 2018, a 273% increase.2 Among youth with complex healthcare needs, it is estimated that approximately 5.6 % have autism spectrum disorder. Existing literature suggests that autistic youth experience significant difficulties interfacing with medical care as compared to their peers who do not meet criteria for ASD. Furthermore, it has been shown that as compared to youth without ASD, youth with ASD have a higher number of medical admissions and increased total medical costs.3 Families with a child with ASD frequently report unmet access to appropriate services or concerns that care is not tailored to their child’s unique needs.1
To date, little research has investigated orthopaedic surgery in patients with co-occurring mental health conditions (e.g., major depressive disorder, anxiety) and neurodivergent identities (e.g., attention-deficit/hyperactivity disorder, intellectual disability).4 The body of literature focusing on providing orthopaedic care to autistic youth is notably limited.5 This is a topic of particular relevance because research has shown that individuals with ASD have lower bone density and are at increased risk of fractures compared to those without ASD.6–9
Each phase of a visit should be considered—anticipation of treatment, the treatment itself, recovery from procedures, adherence to medical care, and pain management. Screening questionnaires have been shown to improve understanding of the patient’s behavioral profile and preferred coping strategies in the ambulatory setting. Other work has explored the use of sensory stimuli in the waiting room and procedure rooms, clear and developmentally appropriate communication with the patient, built-in time for sensory breaks, and family support to manage adherence to recovery, sleep hygiene, and pain management.4,5 Behaviors that are perceived as challenging in autistic children can contribute to stress and overwhelm in their parents, thus increasing parental accommodations of behavior, potentially compromising treatment and recovery.10 Prioritizing training and education for parents of children with ASD can help with minimizing and managing challenging behavior and promoting positive behaviors and interpersonal relationships.10
Taken together, this review fills a gap in the literature regarding orthopaedic care for youth with ASD. Recent surveys of healthcare professionals have revealed a general lack of knowledge about ASD and a desire for additional education. Autism-specific training has been associated with greater levels of comfort working with this population, likely leading to higher quality care.11,12 We present a practical guide for orthopaedic providers in ambulatory and surgical settings so as to improve care for pediatric patients with ASD and their families.
Language
The language we use with our patients and their families is paramount in our ability to connect with and treat all patients. Particularly with pediatric patients with ASD, it is critical that we offer family-centered care informed by current advocacy efforts in the ASD community. Historically, there have been efforts in medicine to use person-first language (PFL) in speaking with patients so as to reduce emphasis on the individual’s disease or disability. The phrase, “child with autism,” is an example of PFL. More recently, there is increasingly recognition in the ASD community that there is a continuum of preferences in terms of identity descriptors, with some individuals preferring PFL, while others would prefer identity-first language (IFL).13 The phrase, “autistic child,” is an example of IFL. Given this variability, during their first encounters with families, providers can ask parents directly about their identity descriptor preferences or take their lead and notice how they speak about their child. In the following paper, we will employ both PFL and IFL as a way to model the variation in preferences across the ASD community.
Optimizing the Orthopaedic Clinic Experience
Preparing for the Visit
Parents play a key role as physicians’ best resources in preparing patients with ASD for a positive medical encounter, particularly because no two children with ASD are the same.2,14,15 While triggers can vary widely, anxiety or sensory processing difficulties can often contribute to sub-optimal treatment adherence in pediatric patients with ASD.16 Collecting information about these triggers ahead of time can help surgeons provide equitable care to their patients with ASD in the orthopaedic clinic.
An introductory phone call prior to the initial visit can help physicians establish a partnership with the patient’s caregivers and begin to understand the patient’s common anxiety triggers and preferred soothing strategies. To anticipate potential triggers during the clinic visit, staff can consider asking about the child’s previous healthcare experiences and discuss any anticipated tasks or procedures during the visit, including laboratory work, radiographs, the application of durable medical products, cast and suture removal, manipulation of fractures, injections, splinting, and casting.5,17 This information will help parents prepare their child for the visit. Physicians can also encourage parents to collaborate with their child’s community treatment team to assist in preparation for the upcoming visit.
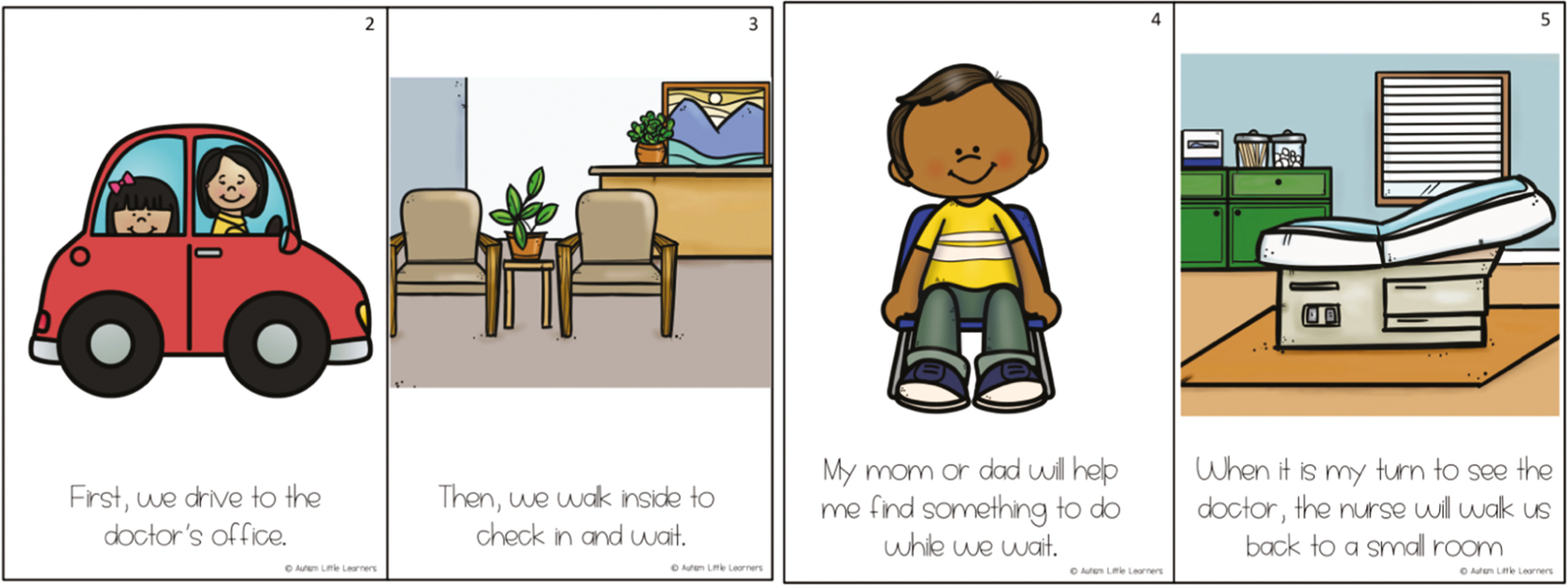
Changes in routine can be particularly stressful for children with ASD, and some youth may benefit from a step-by-step description of the orthopaedic visit.18 One common technique is the use of social stories, which are designed to ease uncertainty by breaking down the encounter into a series of distinct steps using words and photographs.16,19–21 An example of a social story is shown in Figure 1.22 Johnson et al. (2014) found that an iPad application using social stories to describe MRI, CT scan, x-ray, and nuclear medicine procedures reduced parent anxiety and child-externalizing behaviors during imaging visits.23 Healthcare-specific visual aids, including scenes like visiting the hospital for casting, have also been well-received by parents.24
Figure 1. An example of a social story about going to the doctor. From Tara Tuchel, autismlittlelearners.com.
Finally, it is important to ask about any behaviors the child displays when they are having trouble coping, signaling that it may be time to take a break during the exam.25 Parents may also share certain behavioral strategies (such as role modeling, imitation, distraction, and reward systems) that have been used successfully at home or school to encourage cooperation.17,26
Surgical practices may find it helpful to develop a standardized list of questions to ask during these preparatory phone calls. Venkat et al. (2016) shared one example, designed to be used by healthcare teams caring for patients with ASD in the emergency department.27 A copy of the Pediatric Individualized Behavior Checklist developed by Yale-New Haven Children’s Hopsital is also included at the end of the review for reference (Appendix). While this information can be collected by asking parents to fill out a survey in the clinic setting, some parents have expressed concern that physicians will not read the responses and would prefer to discuss the patient’s needs on the phone.14
Day of Visit
Scheduling patients with ASD as the first visit of the day clinic session is an easy way to minimize time spent in the waiting room.5,19,26,28 Allowing parents to fill out paperwork ahead of the visit will afford them a greater ability to focus on their child while in the clinic.26 Caregivers can be encouraged to bring a favorite item for the child (toys, tablets, video games, headphones, etc.) to provide distraction throughout the visit.
Staff should be aware of the patient’s preferred method of communication. In a survey of hospitalized patients with ASD, Kopecky et al. (2013) found that communication strategies varied significantly between patients. More specifically, 23% expressed their needs verbally, 38% used signs or gestures, and 31% used communication tools such as a Picture Exchange Communication System (PECS) or electronic device.29
The physical exam is a common point of difficulty for patients with ASD.25 One study found that half of patients with ASD preferred for the physician to explain each step of the exam before performing it, and approximately one-third preferred to examine the physician’s instruments themselves or have the exam modeled on a trusted adult.29 Distraction can also be helpful; video goggles and handheld video devices have been found to decrease anxiety during a routine visit.30 Physicians should respect self-soothing techniques, such as repetitive motions, and be aware that eye contact may be uncomfortable for the patient. Patience is essential for success, and adequate time should be scheduled for all assessments and procedures to allow for breaks.17
Consensus-based recommendations for sedation in patients with ASD are limited.5 Therefore, the decision to use sedation for imaging or anxiety-inducing procedures, such as cast removal and pin pulling, should be made on an individualized basis, taking into account the risks of performing the procedure without sedation and the inherent risks of sedation itself.16
Restraints should be avoided, whenever possible. Restraints are associated with loss of dignity for the child and can cause psychological and physical harm to both the patient and staff.17,20,31 For patients with ASD, apprehension about medical procedures has been found to increase with age, likely due to prior negative encounters with the healthcare system.29 To facilitate productive interactions with the medical system in the future, physicians should consider delaying non-emergent procedures if behavioral techniques are not sufficient to manage patient distress during the visit.5
Optimizing the Preoperative Experience
Preparing for Surgery
A strong partnership between the surgeon and caregivers will help facilitate an open dialogue about the risks and benefits of surgery. For example, patients with ASD may face specific challenges adjusting to the hospital environment. A recent study by Hazen at al. (2020) reports that patients with a history of self-injurious behavior may be at greatest risk of agitation during the hospitalization.32 Sensory sensitivities were also predictive of agitation during admission. In the context of orthopaedics, this may present as challenges adjusting to wearing a brace or a cast.33
These conversations are especially important in identifying appropriate candidates for complex treatments. One study found that a third of pediatric limb reconstruction patients reported postoperative sleep disturbances and half reported absences from school extending beyond 2 weeks.4 While none of the patients in the study had a diagnosis of ASD, it is important to think about how such a significant change in routine may affect autistic patients considering this type of surgery.
Phone calls to prepare families for surgery can look similar to those used for clinic visits. Parents may want to create social stories to help their child prepare for surgery, and for some patients, a preoperative tour of the facility may reduce anxiety.26 Caregivers should be encouraged to bring a favorite item for comfort and distraction during their child’s time in the hospital.20,25,29,34,35 To help families prepare for surgery, Straus et al. (2019) recommend parents be given written instructions on what to expect during their hospital visit, since verbal instructions can be hard to remember.35 Much like clinic visits, parents report that completing paperwork prior to arrival can help the day run smoothly.26 Discharge education can also be given before the procedure so the parents can focus on the needs of their child postoperatively.36
Day of Surgery
Children with ASD have been found to have higher anxiety in the preoperative holding room than children without ASD undergoing outpatient surgery.37 To facilitate a successful healthcare encounter, physicians can advocate for environmental modifications for their patients with ASD to alleviate some of this anxiety.2 Similar to efforts made in the clinic setting, preoperative modifications should be individualized and informed by conversations with the patient’s caregivers prior to surgery.
Scheduling patients with ASD as the first case of the day helps minimize waiting and NPO periods.19,26,28 The hospital presents patients with several novel sensory stimuli, including the fluorescent lights, beeping monitors, and smell of antiseptics.26 To minimize overstimulation, consider bypassing the typical preoperative waiting room in favor of a quiet room.25,28 Keeping the number of healthcare providers in the room to a minimum can also help ease patients’ anxiety.18,26 Staff should be aware that some patients with ASD will experience difficulty tolerating the continuous monitoring of vital signs. Therefore, when clinically appropriate, consider spot-checking vital signs and clustering nursing interventions to reduce postoperative stimulation.16,25
Previous studies have found that children with ASD have more difficulty with the induction of anesthesia than similarly aged peers without ASD.25,37 To ease the transition into the operating room, oral premedication can be mixed with a favorite drink to mask the unpleasant flavor.18,28 If the patient initially refuses, it may be helpful to have the parent model sharing the drink (minus the medication) with their child.28 Parents should be encouraged to stay with their child until anesthesia is induced.19 If the parent thinks their child will benefit, they can model breathing through the anesthesia mask and the patient can practice breathing through the mask prior to surgery. The patient may need time to adjust to the novelty of the mask and should not be rushed.34
There are a number of steps the surgical team can take to facilitate the postoperative recovery period while the patient is under anesthesia. These include drawing blood for any necessary lab tests and giving prophylactic IV fluids, pain medications, and anti-nausea medications before leaving the OR.36 When clinically appropriate, this can facilitate the early removal of the IV cannula, which may not be tolerated by the patient postoperatively.18
Upon admission, the patient may benefit from the support of a multidisciplinary team. Depending on the needs of the child, the surgeon may consider coordinating with certified child life specialists, occupational therapists, speech and language pathologists, and/or child psychologists and psychiatrists.2,29 Some hospitals even have autism-specific resources. For example, Boston Medical Center recently expanded the role of Autism Resource Specialists, who help coordinate care for patients with ASD in different departments.38
Optimizing the Postoperative Experience
Pain Management
Contrary to previous reports that children with ASD show reduced pain sensitivity, Nader et al. (2004) found that children with ASD displayed significant facial pain reactions to venipuncture.39 While the stress of the hospital environment may trigger behavioral outbursts, physicians should avoid attributing all patient distress to the change in environment. Pediatric patients with ASD may not be able to verbalize their pain, which can lead to undertreatment.34
In interviewing patients with ASD postoperatively, Ely et al. (2016) found that all patients were able to describe and locate their pain using a variety of approaches. Most patients preferred pointing to the pain location and using words, rather than numbers, to describe the intensity of pain. The authors found that parental involvement was essential to interpreting pain words and behaviors.15
Patient Safety
Surveying parents of children with ASD, Kopecky et al. (2013) found that 50% had concerns about their child’s safety in the inpatient hospital setting.29 Specifically, parents expressed concerns about wandering, self-injury, aggression, pica, and pulling out IV tubes. Gearner Thompson and Tielsch-Goddard (2014) found that patients with ASD had particular difficulty waking up from anesthesia surrounded by the extensive sensory stimuli in PACU.25 Therefore, the authors suggest a private recovery room to reduce postoperative agitation. The postoperative area should also have safety rails or padding available.19
If a patient’s behavior is creating a safety risk to the patient or staff, Thom et al. (2020) suggest using medications to calm the patient enough to allow optimal use of behavioral strategies and coping techniques. Literature on the pharmacological management of acute agitation in ASD is notably lacking.2 Therefore, information about a patient’s past responses to medications should guide medication choice. If such information is not available, the authors suggest clonidine or guanfacine for mild to moderate agitation and risperidone or aripiprazole for more severe episodes. Benzodiazepines and anticholinergic medications should be avoided since these medications are associated with an increased risk of paradoxical reactions.2 We believe that if medication is being considered, involvement of the multidisciplinary team referred to earlier is mandatory.
The hospital can be overwhelming, and patients with ASD may especially benefit from recovery in a familiar environment.19 It is recommended that patients be discharged to home as quickly as it is safe to do so.28,34 Conversations about discharge planning should occur preoperatively; we recommend evaluation by a physical therapist to initiate training and ordering of durable medical equipment so this does not cause a discharge delay.
Summary
Communicating with the patient’s caregiver, even prior to the first appointment, can significantly aid in understanding the patient’s stressors so a personalized treatment approach can be developed. Communication of individualized approaches to healthcare teams can help identify appropriate and efficient interventions while ensuring the safety of the patient and staff. Despite its high prevalence, there is little research pertaining to the musculoskeletal care of children with ASD. Future research and education are necessary to improve healthcare equity and provide quality care to children with ASD.
Additional Links
- Autism Speaks: Tool Kits for Healthcare Professionals
- The Centers for Disease Control and Prevention: Information on Autism Spectrum Disorder for Healthcare Providers
- Autism Little Learners: “Going to the Doctor” social story
Disclaimer
No funding was received. The authors report no conflicts of interest related to this manuscript.
References
- Kogan MD, Strickland BB, Blumberg SJ, et al. A national profile of the health care experiences and family impact of autism spectrum disorder among children in the United States, 2005-2006. Pediatrics. 2008;122(6):e1149-58.
- Thom RP, Hazen MM, McDougle CJ, et al. Providing inpatient medical care to children with autism spectrum disorder. Hosp Pediatr. 2020;10(10):918–924.
- Croen LA, Najjar DV, Ray GT, et al. A comparison of health care utilization and costs of children with and without autism spectrum disorders in a large group-model health plan. Pediatrics. 2006;118(4):e1203-11.
- Richard HM, Nguyen DC, Birch JG, et al. Clinical implications of psychosocial factors on pediatric external fixation treatment and recommendations. Clin Orthop Relat Res. 2015;473(10):3154-3162.
- Deon Kidd V, De Claro AMO. Preparing for autistic patients in orthopaedic surgery: tips for a successful health-care interaction. J Bone Joint Surg Am. 2018;100(20):e132.
- Ekhlaspour L, Baskaran C, Campoverde KJ, et al. Bone density in adolescents and young adults with autism spectrum disorders. J Autism Dev Disord. 2016;46(11):3387-3391.
- Neumeyer AM, Gates A, Ferrone C, et al. Bone density in peripubertal boys with autism spectrum disorders. J Autism Dev Disord. 2013;43(7):1623-1629.
- Neumeyer AM, O’Rourke JA, Massa A, et al. Brief report: bone fractures in children and adults with autism spectrum disorders. J Autism Dev Disord. 2015;45(3):881-887.
- Hediger ML, England LJ, Molloy CA, et al. Reduced bone cortical thickness in boys with autism or autism spectrum disorder. J Autism Dev Disord. 2008;38(5):848-856.
- Bearss K, Burrell TL, Challa SA, et al. Feasibility of parent training via telehealth for children with autism spectrum disorder and disruptive behavior: a demonstration pilot. J Autism Dev Disord. 2018;48(4):1020-1030.
- Austriaco K, Aban I, Willig J, et al. Contemporary trainee knowledge of autism: how prepared are our future providers? Front Pediatr. 2019;7:165.
- Wachob D, Pesci LJ. Brief report: knowledge and confidence of emergency medical service personnel involving treatment of an individual with autism spectrum disorder. J Autism Dev Disord. 2017;47(3):887-891.
- Taboas A, Doepke K, Zimmerman C. Short report: preferences for identity-first versus person-first language in a US sample of autism stakeholders. Autism. 2022;0:1-6. doi:10.1177/13623613221130845
- Bultas MW, McMillin SE, Zand DH. Reducing barriers to care in the office-based health care setting for children with autism. J Pediatr Health Care. 2016;30(1):5-14.
- Ely E, Chen-Lim ML, Carpenter KM, 2nd, et al. Pain assessment of children with autism spectrum disorders. J Dev Behav Pediatr. 2016;37(1):53-61.
- Johnson NL, Rodriguez D. Children with autism spectrum disorder at a pediatric hospital: a systematic review of the literature. Pediatr Nurs. 2013;39(3):131-141.
- Souders MC, Freeman KG, DePaul D, et al. Caring for children and adolescents with autism who require challenging procedures. Pediatr Nurs. 2002;28(6):555-562.
- Vlassakova BG, Emmanouil DE. Perioperative considerations in children with autism spectrum disorder. Curr Opin Anaesthesiol. 2016;29(3):359-366.
- Biyani S, Morgan PS, Hotchkiss K, et al. Autism spectrum disorder 101: a primer for pediatric otolaryngologists. Int J Pediatr Otorhinolaryngol. 2015;79(6):798-802.
- Taghizadeh N, Davidson A, Williams K, et al. Autism spectrum disorder (ASD) and its perioperative management. Paediatr Anaesth. 2015;25(11):1076-1084.
- Sansosti FJ, Powell-Smith KA, Kincaid D. A research synthesis of social story interventions for children with autism spectrum disorders. Focus Autism Other Dev Disabil. 2004;19(4):194-204.
- Tuchel T. Going to the Doctor. Available at: https://autismlittlelearners.com/going-to-the-doctor-social-story/.
- Johnson N, Bree O, Lalley EE, et al. Effect of a social script iPad application for children with autism going to imaging. J Pediatr Nurs. 2014;29(6):651-659.
- Vaz I. Visual symbols in healthcare settings for children with learning disabilities and autism spectrum disorder. Br J Nurs. 2013;22(3):156-159.
- Thompson DG, Tielsch-Goddard A. Improving management of patients with autism spectrum disorder having scheduled surgery: optimizing practice. J Pediatr Health Care. 2014;28(5):394-403.
- Selvey P, Stypulkowski K, Waisbren S. Surgical management of the patient living with autism. Surg Open Sci. 2019;1(2):90-96.
- Venkat A, Migyanka JM, Cramer R, et al. An instrument to prepare for acute care of the individual with autism spectrum disorder in the emergency department. J Autism Dev Disord. 2016;46(7):2565-2569.
- van der Walt JH, Moran C. An audit of perioperative management of autistic children. Paediatr Anaesth. 2001;11(4):401-408.
- Kopecky K, Broder-Fingert S, Iannuzzi D, et al. The needs of hospitalized patients with autism spectrum disorders: a parent survey. Clin Pediatr (Phila). 2013;52(7):652-660.
- Isong IA, Rao SR, Holifield C, et al. Addressing dental fear in children with autism spectrum disorders: a randomized controlled pilot study using electronic screen media. Clin Pediatr (Phila). 2014;53(3):230-237.
- Koski S, Gabriels RL, Beresford C. Interventions for paediatric surgery patients with comorbid autism spectrum disorder: a systematic literature review. Arch Dis Child. 2016;101(12):1090-1094.
- Hazen EP, Ravichandran C, Rao Hureau A, et al. Agitation in patients with autism spectrum disorder admitted to inpatient pediatric medical units. Pediatrics. 2020;145(Suppl 1):S108-S116.
- Chambers H, Becker RE, Hoffman MT, et al. Managing behavior for a child with autism in a body cast. J Dev Behav Pediatr. 2012;33(6):506-508.
- Seid M, Sherman M, Seid AB. Perioperative psychosocial interventions for autistic children undergoing ENT surgery. Int J Pediatr Otorhinolaryngol. 1997;40(2-3):107-113.
- Straus J, Coburn S, Maskell S, et al. Medical encounters for youth with autism spectrum disorder: a comprehensive review of environmental considerations and interventions. Clin Med Insights Pediatr. 2019;13:1179556519842816.
- Bevan S, Harris K, Maeder-Chieffo S, et al. Positive healthcare encounters for children with autism spectrum disorder: accommodations during surgical procedures. J Perianesth Nurs. 2022;0:1-6. doi:10.1016/j.jopan.2022.05.070
- Elliott AB, Holley AL, Ross AC, et al. A prospective study comparing perioperative anxiety and posthospital behavior in children with autism spectrum disorder vs typically developing children undergoing outpatient surgery. Paediatr Anaesth. 2018;28(2):142-148.
- O’Hagan B, Friedman A, Bartolotti L, et al. Building an Autism Friendly Hospital: How we started, what we have accomplished, and where we go from here. 2019. https://www.aucd.org/template/news.cfm?news_id=14472&id=17.
- Nader R, Oberlander TF, Chambers CT, et al. Expression of pain in children with autism. Clin J Pain. 2004;20(2):88-97.
Appendix
Pediatric Individualized Behavioral Checklist
BACKGROUND INFORMATION:
Has your child been to the hospital before? □ Yes □ No
IF YES: □ Inpatient Admission □ Outpatient Physician Appointment □ Outpatient Imaging Appointment
□ Emergency Department □ Outpatient Procedure or Surgery
What was your experience: □ Positive □ Negative □ Neutral
How does your child communicate best with others?
□ Speaks in full sentences □ Speaks in short phrases □ is non-verbal □ Uses American Sign Language □ Uses a communication device
□ Pointing/gesturing □ Facial expressions (smiling, frowning…etc.) □ PECS (picture exchange communication system) □ scripting (echolalia)
How does your child best understand information?
□ Spoken language □ Pictures/symbols □ Written words □ Social stories □ Visual schedules
□ First/then commands □ Combination of verbally and visually presented information
□ Other__________________________________________________
How does your child communicate that they are in pain?
□ Using pain scales □ Using pain communication boards □ Verbalizing pain □ Self-Injurious Behavior
□ Increasing repetitive behaviors □ Pointing or pulling at body □ Becoming quiet □ Withdrawing
□ Increased activity □ Agitation and Aggression □ Bolting or attempts to escape □ Screaming
□ Other_______________________________________________________________
BEHAVIORAL INFORMATION:
Safety Concerns and behaviors to be aware of- Does your child:
□ Self-harm □ Acts aggressively towards others □ Tries to leave the room □ Destroys property
□ Falls to the ground □ Pulls medical equipment off □ Repetitive behaviors/Stereotypies (rocking, flapping)
□ Repetitive language □ Repetitive questioning □ Blank stare/becoming quiet
□ Verbal aggression □ Withdrawal from situations
Other______________________________________________________________
The below are potential triggers or areas of difficulty for my child:
□ Strong smells □ Bright lighting □ Physical touch □ Texture (food, clothing)
□ Noise □ Large groups of people □ Small spaces □ Presence of strangers □ Parental separation
□ “White coats” (physician attire) □ Caregivers of a certain gender
□ Rapid transitions □ Removal of items without preparation
□ When immediate demands are not met □ Pain/discomfort □ Constipation □ Hunger
□ Other____________ □ If yes to any of the above, please describe______________________
If your child is triggered, how likely is that s/he may escalate to the point of exhibiting significantly impairing behaviors?
□ Very likely
□ Somewhat likely
□ Somewhat unlikely
□ Minimally likely
The below part(s) of the medical exam are/have been upsetting to my child:
□ Pulse oximetry (finger clip or sticky probe on finger or toe)
□ Blood pressure cuff
□ Eye, ear or mouth exam (exam using an instrument)
□ Taking Medication
□ Physical exam
□ Diagnostic imaging (x-ray, CT scan, MRI)
□ Blood draws, finger sticks, IV start, etc.
□ Transportation in a stretcher or wheelchair
□ Height/Weight Measurements
□ Other
Toileting Habits
□ Uses bathroom independently □ Needs assistance with bathroom/has accidents
□ Uses pull up/diaper, etc. □ Fecal smearing
□ Prone to constipation □ Difficulty with toileting hygiene
□ Voiding on Floor □ Other toileting concerns
Eating/Food Preferences (Please bring any special utensils required for eating from home)
□ Feeds themselves
□ Requires help to eat
□ Has oral aversions
□ Parental preference for specialized diet (i.e.: parent prefers ketogenic or gluten free diet)
□ Has limited food preferences
COPING AND DE-ESCALATION STRATEGIES
The below coping and de-escalation strategies work best for my child:
□ Use simple, direct language □ Use ONE VOICE □ Provide 2-3 choices
□ Presence of specific caregiver □ Redirection □ Use of Social Stories
□ Use of First/Then Language □ Visual Cues □ Model any necessary procedures
□ Keep lights dimmed □ Keep noise levels low □ Counting
□ Give ‘2 minute’ warning before changes/transitions □ Singing/music
□ Food and edible reinforcers
□ Deep breathing
□ Reward system/Behavioral Plan
□ Only do vital signs if necessary
□ Media: TV/Ipad/Phone Distraction
□ Physical touch
□ Allow time for processing questions or instructions
□ Minimize the time between arrival at the hospital and time of surgery/appointment
□ Use calm, soft tone of voice when speaking □ limit eye contact and use neutral facial expressions
□ Other _____________
Sensory coping tools my child uses include: (Please bring any chew tools your child utilizes from home)
□ Weighted blankets □ Fidget toys □ Noise cancellation headphones □ Rocking/movement toy
□ Light toys □ Sound toys □ Electronics □ Soothing Music □ Comfort Item/Transitional Item
□ Sunglasses □ Chewy Snacks □ Other______________________
Preferred comfort/pain management options:
□ Premedication for procedures, IVs, blood draws
□ EMLA/LMX Cream (3 months and above): topical numbing cream “lotion” that sits on the skin for minimum of 30 minutes; must be applied with tegaderm
□ Pain Ease: cold numbing spray that feels like an ice cube on their skin to numb the skin
□ Buzzy: Vibrating bumble bee that sits by the site being attempting for blood draw or IV insertion
□ None of the above
□ Other: ____________
Medicine taking is stressful for my child
□ Yes □ No
IF YES: My child takes medicine best by:
□ Liquid in a spoon □ Liquid in a cup □ Liquid in a syringe □ Pills □ Shots/Injection
□ Pills Crushed into soft substance (applesauce, puddling, etc.) □ Orally disintegrating □ Chewable
Medications to avoid: ___________________
Has your child ever used a pre-med or medication to control or de-escalate behavior?
□ Anti-Anxiety □ Anti-Psychotic □ other ___________________
To be assessed and completed by hospital staff only:
Recommended accommodations based on information obtained above:
□ Requires sensory tool kit
□ Use special entrances
□ Child Life presence
□ Decrease wait times
□ Avoid waiting room/
□ Limit caregivers
□ Keep lighting dim
□ Expedite check-in and check-out
□ Parking accommodations (meet/escort family when possible)
□ Protective Service presence
□ Requires behavioral plan (consult Child Psych or DBP services)
□ Requires additional time/preparation for transitions
□ Limit vital signs and physical exam
□ Board to post visual schedules available
□ Requires access to social stories
□ Requires special escort to pediatric floors
□ Primary nursing
□ Availability of sitters
Courtesy of Yale-New Haven Children’s Hospital