
Current Concept Review
Two Sides to Every Conversation: Communication Strategies and Appropriate Interpreter Utilization in Pediatric Orthopaedics
1University of Wisconsin, Madison, WI; 2Albert Einstein School of Medicine, Bronx, NY; 3Nicklaus Children’s Hospital, Miami, FL
Correspondence: Laura L. Bellaire, MD, University of Wisconsin, 1685 Highland Ave, 6th floor, c/o Kim Stace, Madison, WI 53705. E-mail: [email protected]
Received: January 10, 2023; Accepted: January 10, 2023; Published: February 1, 2023
Volume 5, Number 1, February 2023
Abstract
Marginalized patients including those with limited English proficiency (LEP) are at risk of seeing graver health outcomes across many specialties. Communication barriers contribute to impaired shared-decision making and missed education opportunities. Tools are available to clinicians to allow for more accurate and effective education and to facilitate shared decision-making. This article reviews existing guidelines for utilization of professional interpreters. A framework is provided for pre-visit planning, facilitating appropriate introductions, and setting up a clinic room to optimize workflow. Suggestions are provided for utilizing professional interpreters efficiently and prioritizing patient autonomy, respect, and mutual understanding. Pediatric orthopaedic surgeons and providers can promote health equity by utilizing professional interpreters and using other strategies to communicate effectively with patients and families from diverse backgrounds and/or those who have LEP.
Key Concepts
- Pediatric orthopaedic surgeons can take a leading role in exemplifying the delivery of equitable care, investing in appropriate educational resources in a wider variety of languages and connecting with community resources to improve access for underrepresented communities.
- The use of non-professional interpreters such as relatives, friends, children, or bilingual staff is a breach of the duty of care owed to the patient with potential legal ramifications.
- Professional interpreters work under established standards of practice and ethical guidelines to guide interactions with clear priorities of maintaining accuracy, confidentiality, impartiality, and respect.
- Avoid the temptation to look at the interpreter during a clinic visit rather than the patient or caregiver—remember that they are sharing your words with the patient.
- Language access alone will not erase existing health disparities, but it is a critical step toward optimizing patient outcomes.
Introduction
Communication between people speaking different languages has been an intrinsic part of human history. The presence of interpreters has been critical to many key events in history from peace negotiations to trials for crimes against humanity. In the clinical setting, effective communication hinges on accurate delivery of information between parties. When language or cultural discordance exists between a patient, their caregiver, and/or a medical provider, utilizing a professional interpreter allows for accurate passage of information, which in turn facilitates further discussion and shared decision-making.
Culture is best described as a lens through which individuals can express a “sense of identity, belonging, and continuity” that facilitates relationships and interaction within a group.1 This lens of culture is not static but dynamic, and the differences within an identifying culture can be expected based on generation, location, and current events. Culture may overlap with some ethnic and racial groups, may cut across these groups, may be limited to subpopulations, and may apply to groups defined by neither ethnicity nor race.2 Assuming that individuals who speak the same language or are from the same racial or ethnic group all share the same cultural beliefs is a harmful oversimplification.
Across specialties, marginalized communities, including limited English proficient (LEP) patients and families, still have decreased access to preventive care, less treatment for chronic conditions, and increased emergency room visits. As a result, they see graver health outcomes and increased likelihood of developing cardiovascular disease, mental illness, diabetes, and advanced cancers.3–5 There exists clear and substantial value in the pursuit of health equity through appropriate communication with patients and families from diverse backgrounds and/or those who have LEP.
Efforts to improve health equity can and should be far-reaching and inclusive. This article aims to provide several tools to clinicians interested in improving their relationships with patients through language, cultural awareness, and trust. Clinicians have an opportunity to develop connections with patients and their families by being mindful of their own personal implicit and explicit bias, utilizing interpreters effectively when indicated, and using verbal and non-verbal communication tools to establish common ground and shared goals.
Body
Representative Case Example
In order to illustrate how language impacts pediatric orthopaedic patients, families, and clinicians, we will describe a representative clinical scenario:
A 3-year-old female presents as a new patient with bilateral high riding hip dislocations. She is accompanied by her 12-year-old brother and their parents. The family speaks a language for which there is no in-person interpreter at your hospital, so a professional interpreter is made available over the phone. The patient’s older sibling speaks English fluently, and you begin a conversation with him in English. Happy to avoid the additional step of accessing a phone interpreter, you let the older sibling interpret your words for his parents and sibling. Is this appropriate?
If you answered “YES,” did you consider that you are potentially accepting that:
- the sibling may bias the conversation based on his preferences for his family.
- the sibling may intentionally or unintentionally omit information or elaborate.
- this places an unfair burden on the sibling, who is a minor.
- this situation may disrupt family hierarchy and traditional roles or respect.
Clinicians must find ways to develop trust and respect with a patient and their family while also ensuring accurate exchange of information. The use of non-professional interpreters such as relatives, friends, children, or bilingual staff is a breach of the duty of care owed to the patient. In some settings, doing so presents potential legal ramifications.6 If a family member or sibling is fluent, this can be a valuable addition to a visit. The bilingual family member should be reassured that their role as a support person is very important and they can remain in the room and fully participate in the encounter while the professional interpreter conveys the information exchanged accurately and completely without editing or additions.
Pre-Visit Planning
Clinic flow can be impacted by a variety of factors including the incorporation of professional interpreters. Scheduling patients who need interpreter services consecutively can be considered to improve efficiency. Newer time-based billing options place value on spending extra time with patients to ensure communication and education opportunities are optimized and questions are answered. Institution and insurance-specific policies should be queried to ensure visit time is billed appropriately based on existing guidelines, with or without the need for interpreter services. Availability of funding for language access services varies depending on practice setting. Clinicians should consider involving multi-provider teams: designating physician-specific tasks, nursing-specific tasks, and engaging other appropriate staff to allocate time most appropriately. When professional interpreters are incorporated into our clinics seamlessly, they allow us to hear the needs of our patients more clearly and efficiently.
Appropriate Introductions
The first step towards an effective encounter is establishing transparency about the role of each individual in the room and understanding what support is needed to facilitate clear, comprehensible, and accurate communication. The Electronic Medical Record (EMR) helps provide baseline language-proficiency information but depending on the systems in place, may not be accurate or up-to-date. Ultimately, it is the treating clinician’s responsibility to clarify patient and family language proficiency and other preferences. For example, ask the patient, “In what language do you prefer to discuss your healthcare?” For patients that are minors or incapacitated, the preferred language of the patient’s parent, guardian, or surrogate decision-maker should also be determined.7 Additional support should similarly be offered to patients with hearing, visual, or speech impairments, but that is beyond the scope of this article.
Beginning the visit with a clear and concise introduction of yourself and any trainees or other staff members in the room is necessary. Your introduction should include your title, name, and your role in the visit. For example, “I am Dr. X. I am a pediatric orthopaedic surgeon, and I am here to conduct the visit for you/your child today.” If an interpreter is present in the room, turn or gesture so that they interpret your introduction and proceed to introduce themselves immediately so that they may establish their role, privacy expectations, and proceed to interpret for the remainder of the visit. If you have conversational abilities in the patient’s language, this does not negate the need for a professional interpreter. Next, you may introduce other trainees/individuals and their roles or give them opportunities to do so.
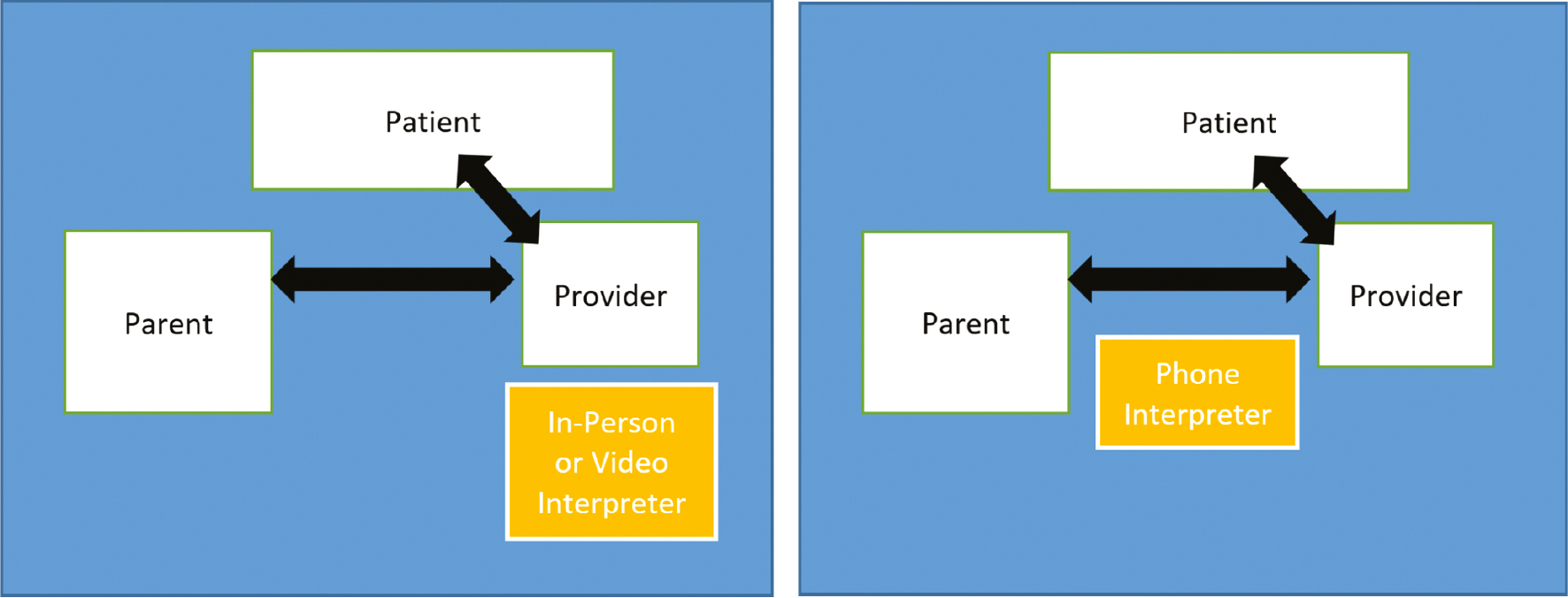
If the interpreter is physically present or visible via a video platform, position yourself adjacent to them so you are both facing the patient directly and not facing each other (Figure 1). If the interpreter is present only by telephone or audio, placing this device between you and the patient/family so both parties can easily hear and both are directed toward each other and the source of audio is most appropriate. Take a moment to reorient the room appropriately before proceeding (Figure 2).
Figure 1. Set up your clinic room for success. Here, the physician is seated close to the patient, facing him and his caregiver. The professional interpreter is present via video and is positioned adjacent to the physician, facing the patient and caregiver as well. The clinician should make eye contact with the individual they are addressing, not the interpreter.

Figure 2. Diagram of room setup suggestions for in-person, video, and phone interpreters. The left diagram shows a parallel seating arrangement: the clinician faces the patient and caregiver, speaking to them directly. The interpreter is positioned so as to speak directly to the patient and caregiver, parallel with the clinician or slightly set back behind the clinician allowing unimpeded face-to-face conversation between the clinician and patient/caregiver. The right diagram shows a triradic interview arrangement: the phone is positioned between the provider and the patient/caregiver so that all parties face each other and can easily hear the interpreter’s voice.8
Next, it is important to allow the patient and each family member and visitor to introduce themselves and state their relationship to the patient. If the patient is able to introduce their family members and visitors, this is a helpful way to gauge family dynamics. Once this is complete, it is important to acknowledge each person, demonstrating respect and appreciation for their presence at the visit. If any single individual is withdrawn or does not engage, this is a great opportunity to offer additional services for the visit. Ask a general question, “Is there anything else the hospital/clinic should be aware of to improve your care experience?” Invite other needs or services from the family prior to proceeding, including cultural or religion-based modesty concerns or need for certain garments.7
Tips for Collaborating with an Interpreter
The National Council on Interpreting in Health Care has established standards of practice and ethical guidelines to guide interactions with clear priorities of maintaining accuracy, confidentiality, impartiality, and respect.9,10 The role of the interpreter is to interpret and provide information as it is presented to them by the clinician or the patient, not to assume the roles or responsibilities of other hospital staff and not to speak for the patient or explain medical information to the patient.
Having completed introductions and established the role and position of the interpreter in your visit, the next step is using clear and concise language throughout the visit. Clarify the reason for the visit:
- Rather than relying on the documented chief complaint, begin with an open-ended question to invite the patient’s primary concern(s).
- Follow up by asking them to state their priorities for their visit.
- Make eye contact with the other family members and visitors and ask for any additional concerns, allowing each a voice.
Proceed with gathering the remainder of the patient’s history using the following tips:
- Keep your comments and questions to 1-2 sentences each to allow more “real-time” interpreting to the family and to enhance accuracy.
- Use specific language rather than overly broad terms and analogies. A professional interpreter will ask for clarification if there is not a direct translation.
- For key points, pause to ask or allow for questions.
- If apparent confusion develops on behalf of the patient or the interpreter, ask them to repeat back what they heard or understand to correct misconceptions immediately.
- Avoid the temptation to look at the interpreter/video screen/phone. Remember that they are sharing your words with the patient.
Before you begin the exam:
- State that you are going to examine the patient to better understand the problem at hand.
- Clarify what body parts you will examine. If any sensitive exam maneuvers are needed (removal or shifting of undergarments, rectal exam, etc.), clearly state the need for these maneuvers and why they are relevant to the problem at hand. This is an opportunity to offer a female or male chaperone.
- Ask any superfluous individuals to leave the room to facilitate privacy. Ask the patient who, if anyone, they would like to remain in the room during the exam.
- Offer appropriate garments (gowns, shorts, etc.) to allow as much modesty as possible. If a patient prefers to remain in their own garments, acknowledge that this is acceptable but may limit your exam.
- Obtain verbal consent from the patient and the family to proceed.
- Point out relevant exam findings as you go. “You can see a prominence of the ribs when your child bends forward.”
As you discuss the diagnosis or potential diagnoses and next steps:
- Share radiographs, MRI images, and other images with the patient and family where possible.
- Provide brief descriptions of images, pointing to one structure at a time, pausing to allow the interpreter to describe each structure you mention before pointing to the next structure.
- Provide a summary of the family’s listed concerns that they expressed at the beginning of the visit. For each concern, provide a brief explanation: “Your concern about your child’s gait may be explained by their hip dislocation.”
- Provide a list of next steps if further workup is needed.
- Assess the literacy level of patient and family in the non-English language and provide educational materials in the appropriate language(s) whenever possible.
- Appropriate online resources can often be translated within the web browser or with select online applications. You can also suggest to the patient and family that they can audio record the instructions as they are being given on their smartphone.
- If you perceive discomfort or difficulty with any aspect of the visit, it is appropriate to acknowledge this and ask for their input about how to make that better for their next visit.
After the visit with the patient concludes:
- Ask the interpreter to clarify any confusion that arose during the visit. Solicit the interpreter’s feedback about how to make the next visit smoother or more efficient.
- Contact your hospital’s Language Access/Interpreter Services Department to ask whether there are community resources or language appropriate materials you could incorporate in future visits.
Opportunities for Education, Leadership, and Research
The patient population served by orthopaedic surgeons is becoming more diverse, but this is not yet reflected in our workforce. Between 2014-2018, white surgeons constituted 77% of the surgical workforce. Black and Hispanic/Latinx surgeons made up 2% and 3%, respectively.11 Roughly 50 million Americans speak a language other than English at home, and half of those individuals self-identify as speaking English “less than very well.”12 Language discordance is a frequent cause of miscommunication and frustration between patients and clinicians. This impedes shared decision-making and contributes to health disparities. Ultimately, professional interpreters help close the gap, but there is no substitute for language concordance between patients and clinicians.13–18 Medical schools and training programs are recruiting underrepresented minorities, but the slow surgical pipeline—with training spanning over a decade for many surgical specialties—does not lend itself to adjusting quickly.
Short of recruiting physicians from a greater diversity of cultural and language backgrounds, individuals and institutions should focus on developing reliable and valid tools specific to healthcare and individual subspecialties to ensure provision of equitable care. Many medical schools and training programs already offer health equity curriculum line items, but the challenge remains of integrating health equity into the delivery of health services at every level. Linking language spoken by patient with organizational performance measures is a powerful driver for change. Many health systems now report their performance measures disaggregated by Race, Ethnicity and Language (REaL).
We must recognize that language access alone will not erase health disparities. Pediatric orthopaedic surgeons can take a leading role in exemplifying the delivery of equitable care, investing in appropriate educational resources in a wider variety of languages, and connecting with community resources to improve access for underrepresented communities. Further research and work is needed to increase patient education materials covering a wider range of orthopaedic topics in a greater variety of languages. Currently, the POSNA-sponsored OrthoKids website offers both English and Spanish options for many diagnoses as well as education around safety-related topics, surgical information, and fracture care. This could be expanded upon to include a greater variety of languages and topics.
Summary
Communication is the key to trust building with patients and families and to attaining good health outcomes. Addressing the communication needs of LEP patients through the use of professional interpreters is one of the basic and essential must-do’s in healthcare delivery if we are serious about providing equitable care and eliminating disparities. If we can be patient, flexible and willing to learn from others, we empower and maintain the dignity of our patients and we grow into better clinicians and teachers.
Additional Links
- U.S. Department of Health & Human Services, Think Cultural Health: Working Effectively with an Interpreter
- POSNA OrthoKids offers a variety of patient education topics in either English or Spanish, using the drop-down menu. These pages can be translated to other languages using web browser translate functions and applications.
Disclaimer
The authors have no conflicts of interest to report.
References
- Cortis JD. Culture, values and racism: application to nursing. Int Nurs Rev. 2003;50(1):55-64.
- McFarland K, Rhoades D, Roberts E, et al. Teaching communication and listening skills to medical students using life review with older adults. Gerontol Geriatr Educ. 2006;27(1):81-94.
- Kutalek R. Diversity competence in medicine: equity, culture and practice. Wien Klin Wochenschr. 2012;124 (Suppl 3):3-9.
- Chatterji P, Joo H, Lahiri K. Beware of being unaware: racial/ethnic disparities in chronic illness in the USA. Health Econ. 2012;21(9):1040-1060.
- Castillo RJ, Guo KL. A framework for cultural competence in health care organizations. Health Care Manag (Frederick). 2011;30(3):205-214.
- Rights OoC. Civil Rights Requirements-A. Title VI of the Civil Rights Act of 1964, 42 U.S.C. 2000d et seq. (“Title VI”). U.S. Department of Health & Human Services; 2022. Available at: https://www.hhs.gov/civil-rights/for-individuals/special-topics/needy-families/civil-rights-requirements/index.html.
- Commission TJ. Advancing Effective Communication, Cultural Competence, and Patient- and Family-Centered Care: A Roadmap for Hospitals. Oakbrook Terrace, IL: The Joint Commission; 2010. Available at: aroadmapforhospitalsfinalversion727pdf.pdf (jointcommission.org).
- Working with an Interpreter: Roles of an Interpreter and the Triradic Interview. Department of Health and Human Services. Available at: WorkingWithAnInterpreter.pdf (hhs.gov).
- Care TNCoIiH. A National Code of Ethics for Interpreters in Health Care. The National Council on Interpreting in Health Care Working Papers Series; 2004. Available at: Microsoft Word - National Code of Ethics for Interpreters in Health Care.doc (ncihc.org).
- The NCIH. National Standards of Practice for Interpreters in Health Care. NCIHC Brochure; 2005.
- Noel OF, Berg A, Onyango N, et al. Ethnic and gender diversity comparison between surgical patients and caring surgeons. Plast Reconstr Surg Glob Open. 2020;8(10):e3198.
- Survey USCBAC. American Community Survey 1-Year Estimates, S1601. Language Spoken at Home. Washington, DC: U.S. Census Bureau. 2008. Available at: S1601: LANGUAGE SPOKEN AT HOME - Census Bureau Table.
- Carrasquillo O, Orav EJ, Brennan TA, et al. Impact of language barriers on patient satisfaction in an emergency department. J Gen Intern Med. 1999;14(2):82-87.
- Menendez ME, Loeffler M, Ring D. Patient satisfaction in an outpatient hand surgery office: a comparison of english- and Spanish-speaking patients. Qual Manag Health Care. 2015;24(4):183-189.
- Flores G. The impact of medical interpreter services on the quality of health care: a systematic review. Med Care Res Rev. 2005;62(3):255-299.
- Karliner LS, Jacobs EA, Chen AH, et al. Do professional interpreters improve clinical care for patients with limited English proficiency? A systematic review of the literature. Health Serv Res. 2007;42(2):727-754.
- Green AR, Ngo-Metzger Q, Legedza AT, et al. Interpreter services, language concordance, and health care quality. Experiences of Asian Americans with limited English proficiency. J Gen Intern Med. 2005;20(11):1050-1056.
- Hemberg JAV, Vilander S. Cultural and communicative competence in the caring relationship with patients from another culture. Scand J Caring Sci. 2017;31(4):822-829.